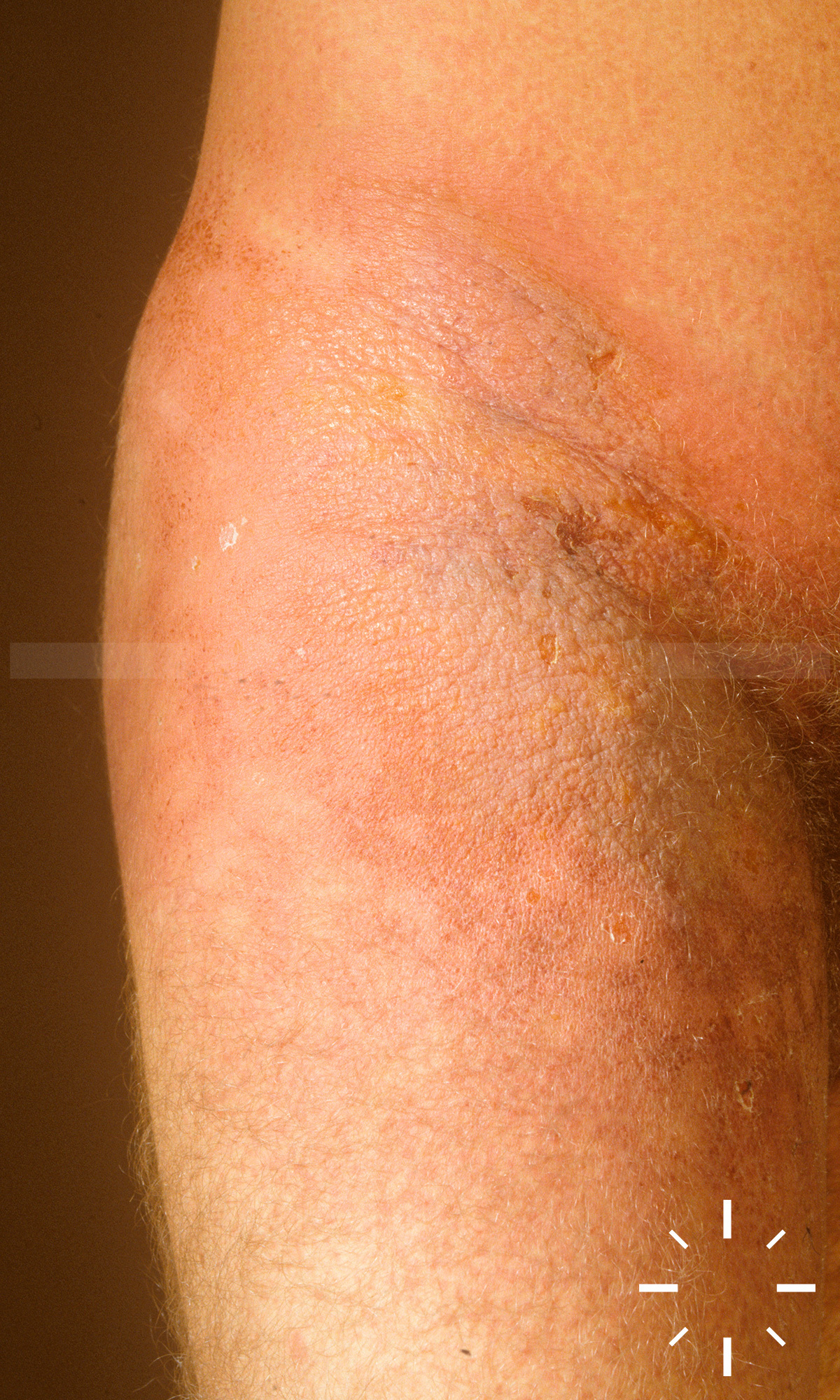
Staphylococcal scaled skin syndrome (SSSS)
Zuletzt aktualisiert: 2022-11-16
Autor(en): Anzengruber F., Navarini A.
ICD11: EA50.2


1/3