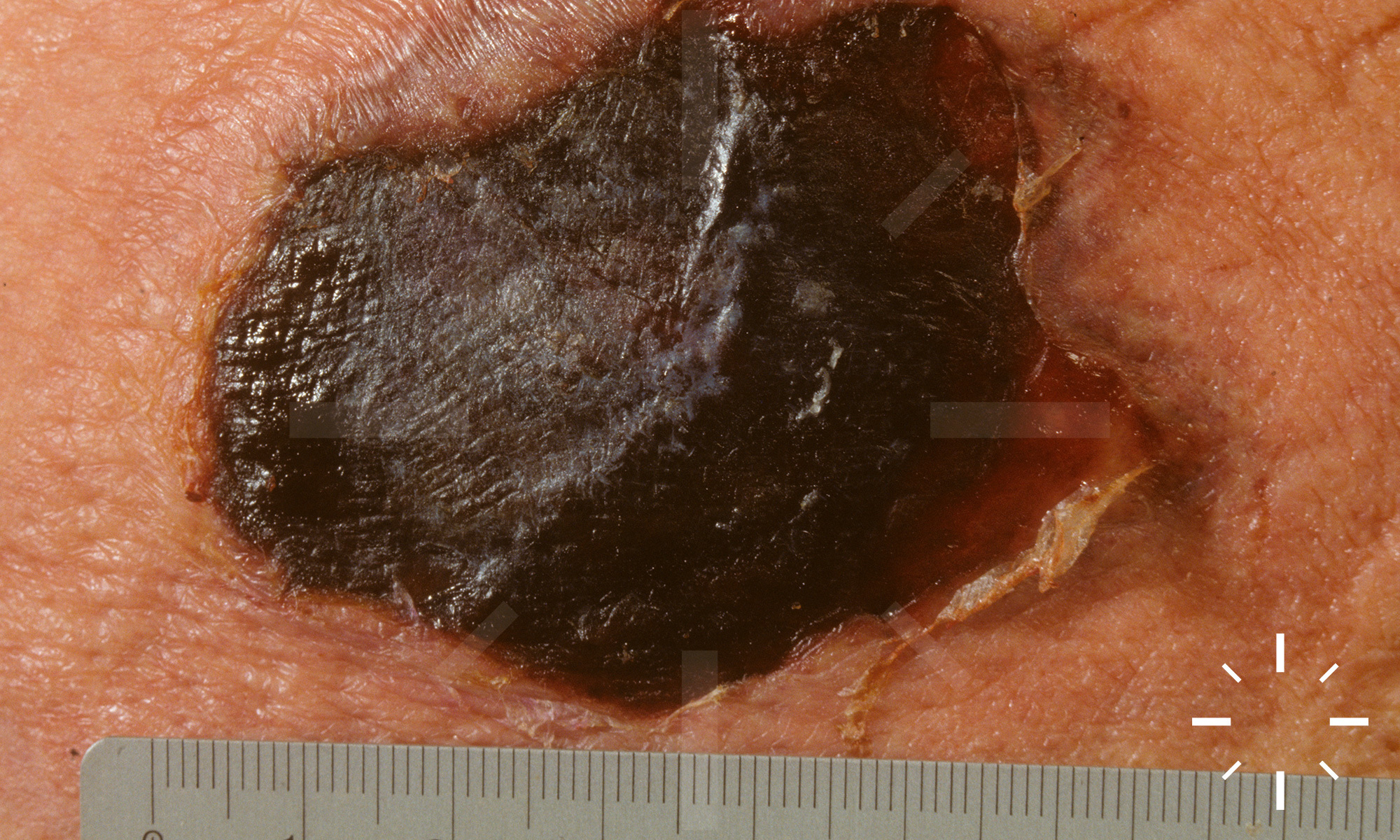
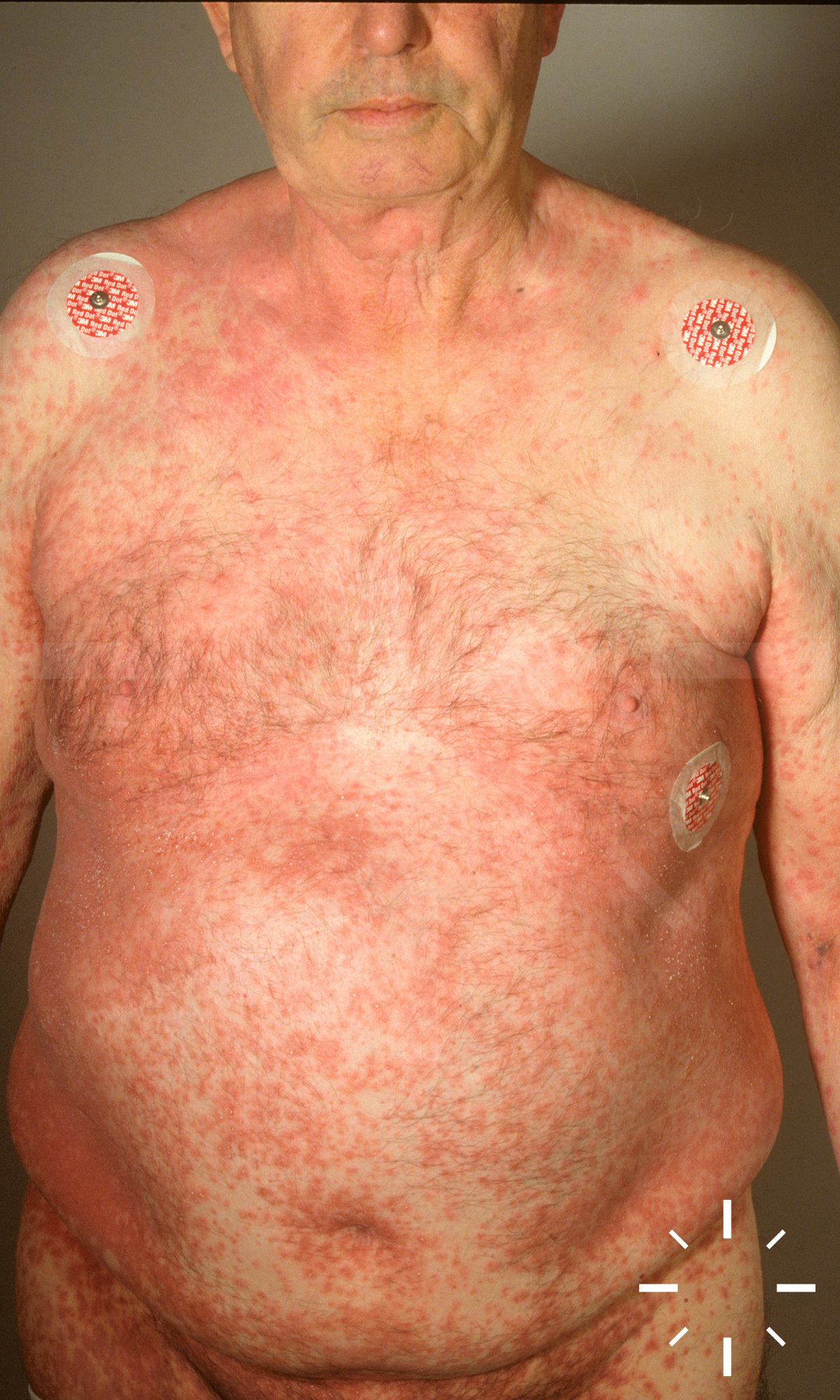
Stevens Johnson Syndrom und toxische epidermale Nekrolyse
Zuletzt aktualisiert: 2022-11-16
Autor(en): Anzengruber F.
ICD11: EB13.2











1/13