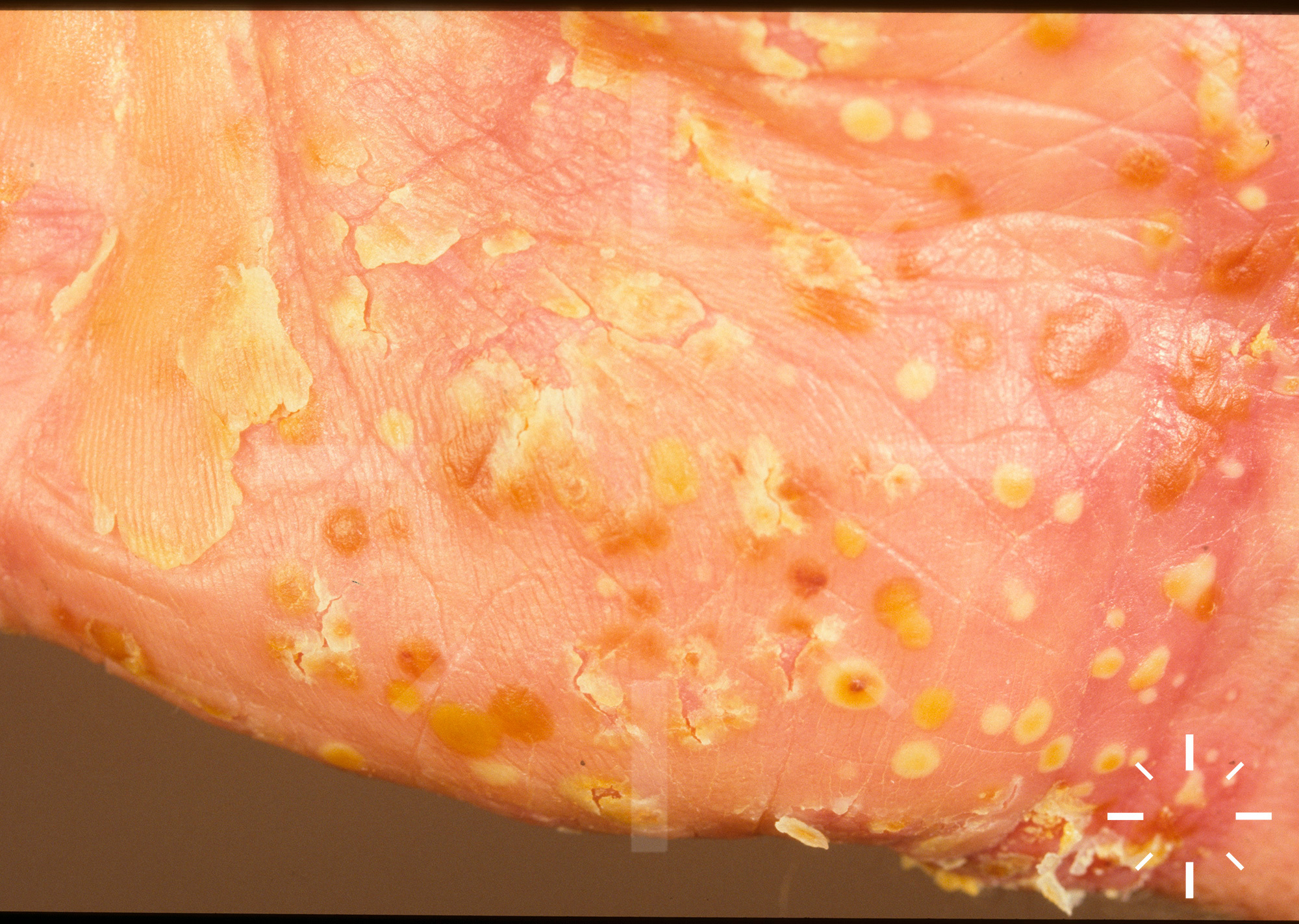
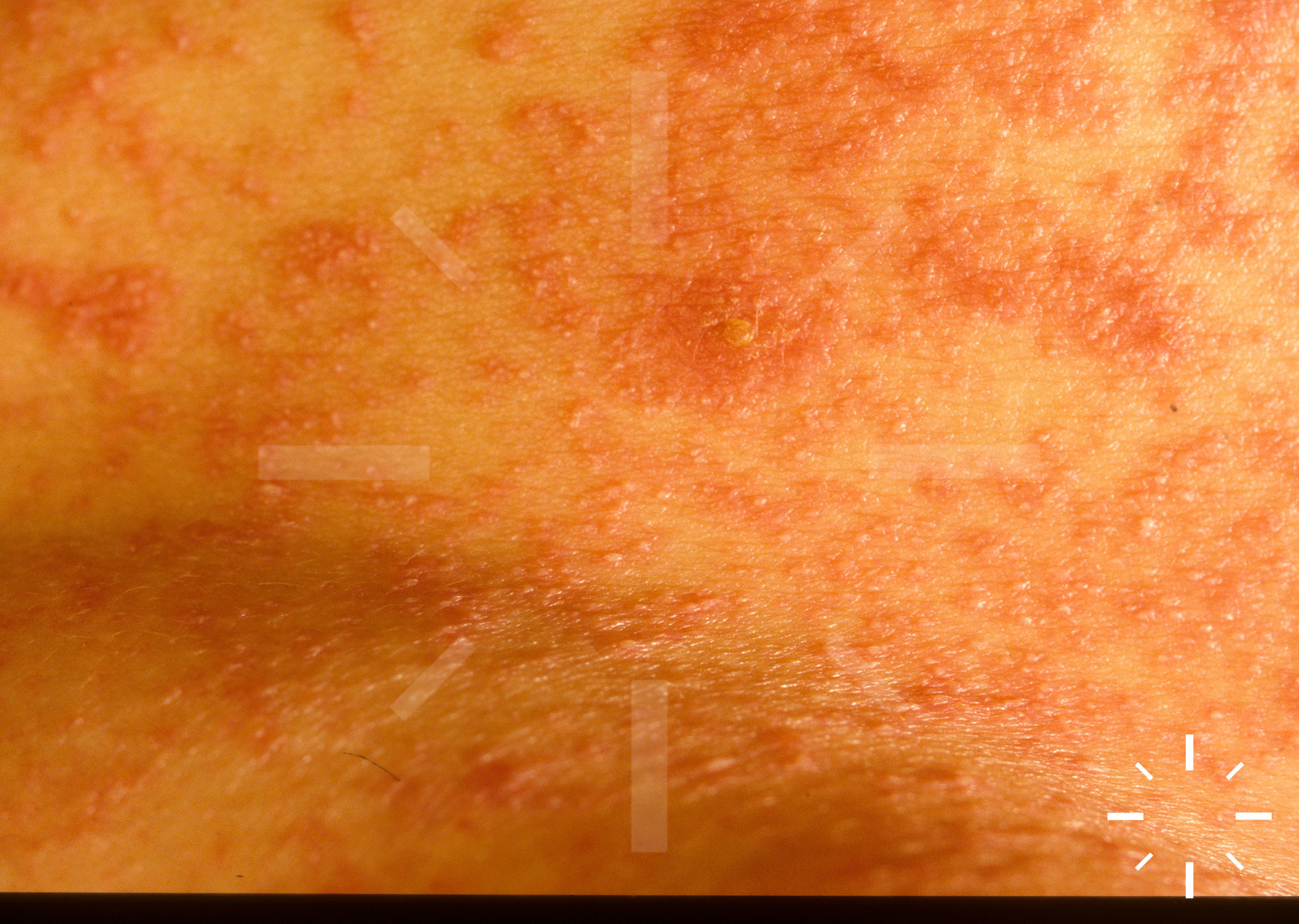
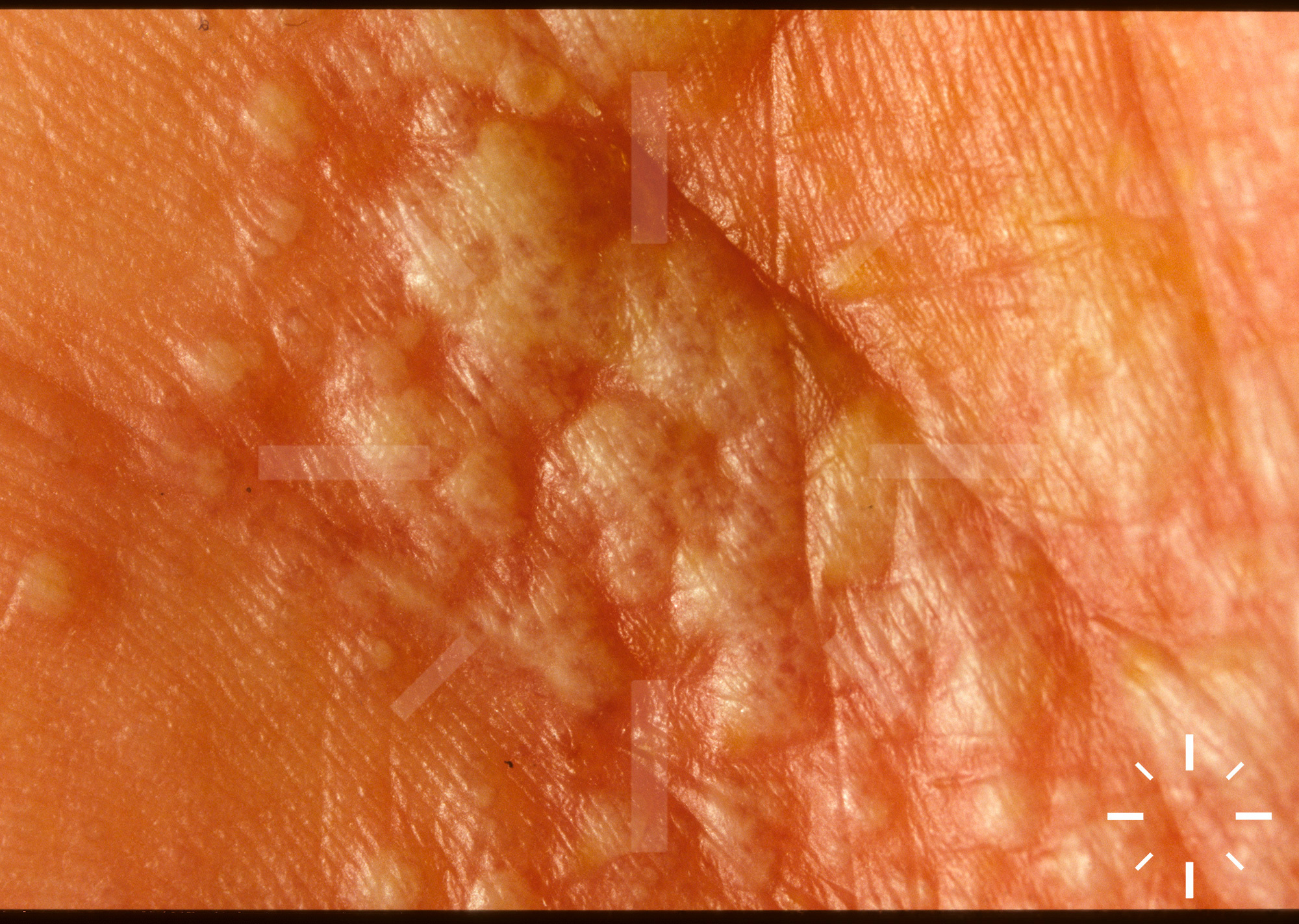
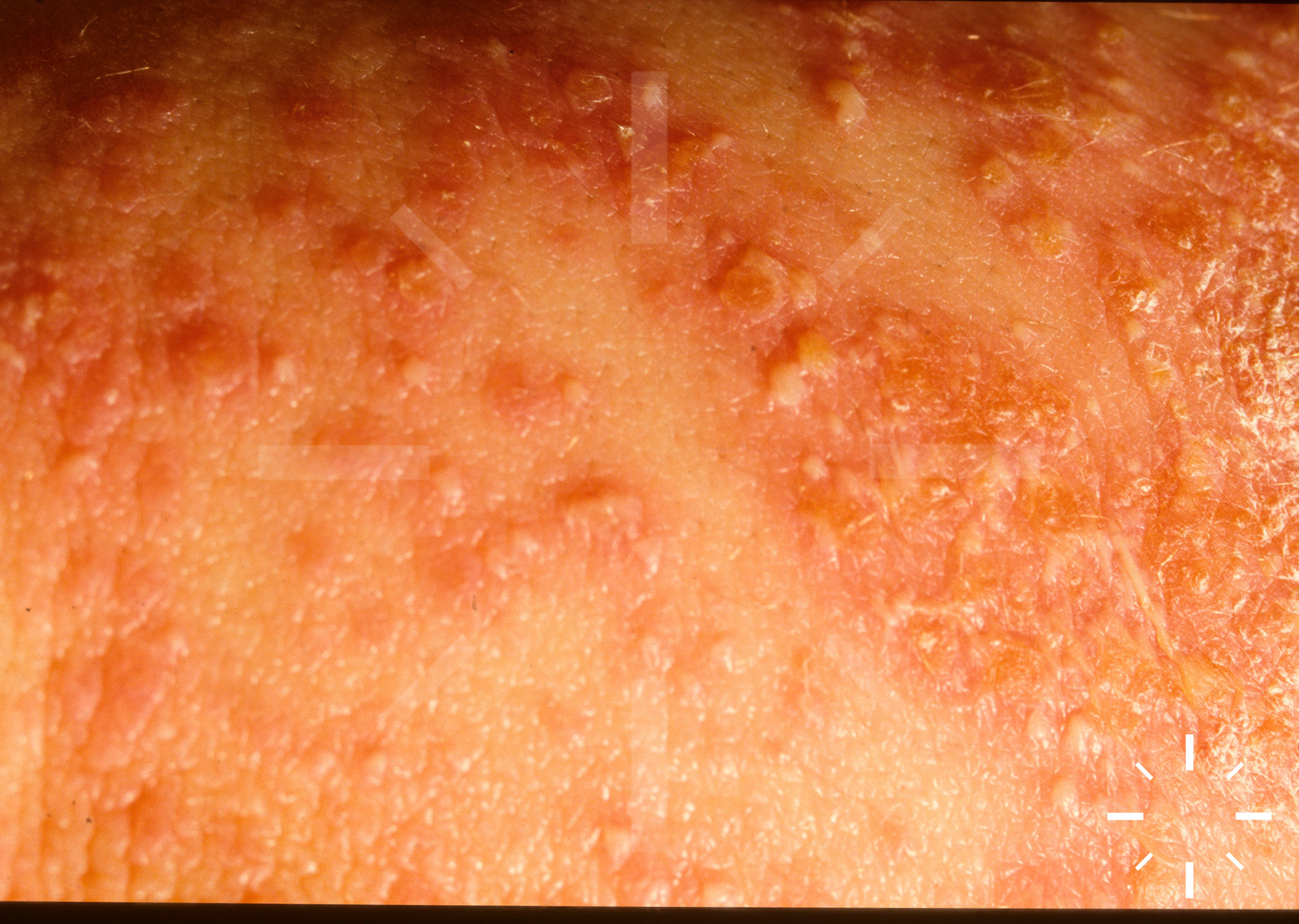
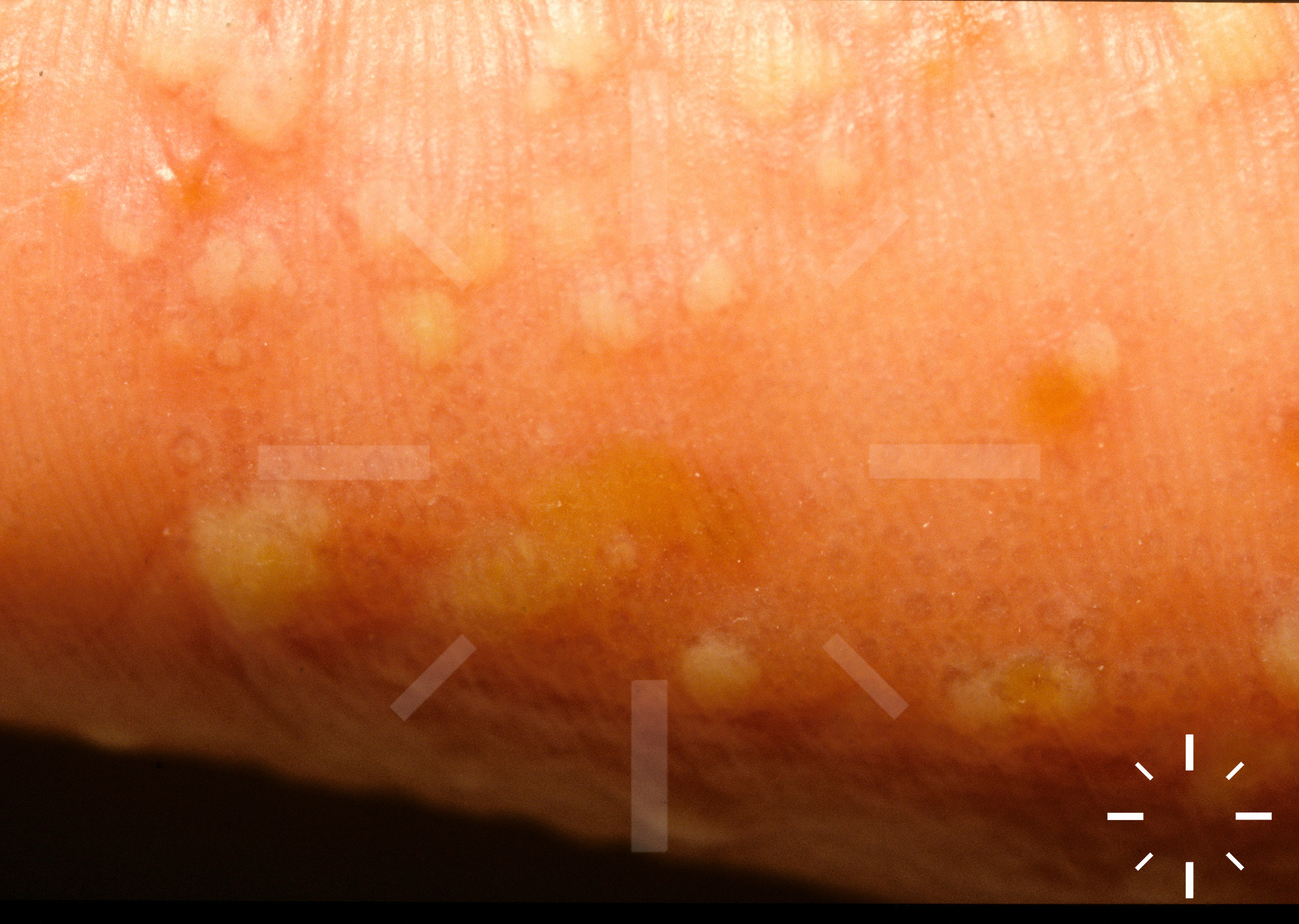
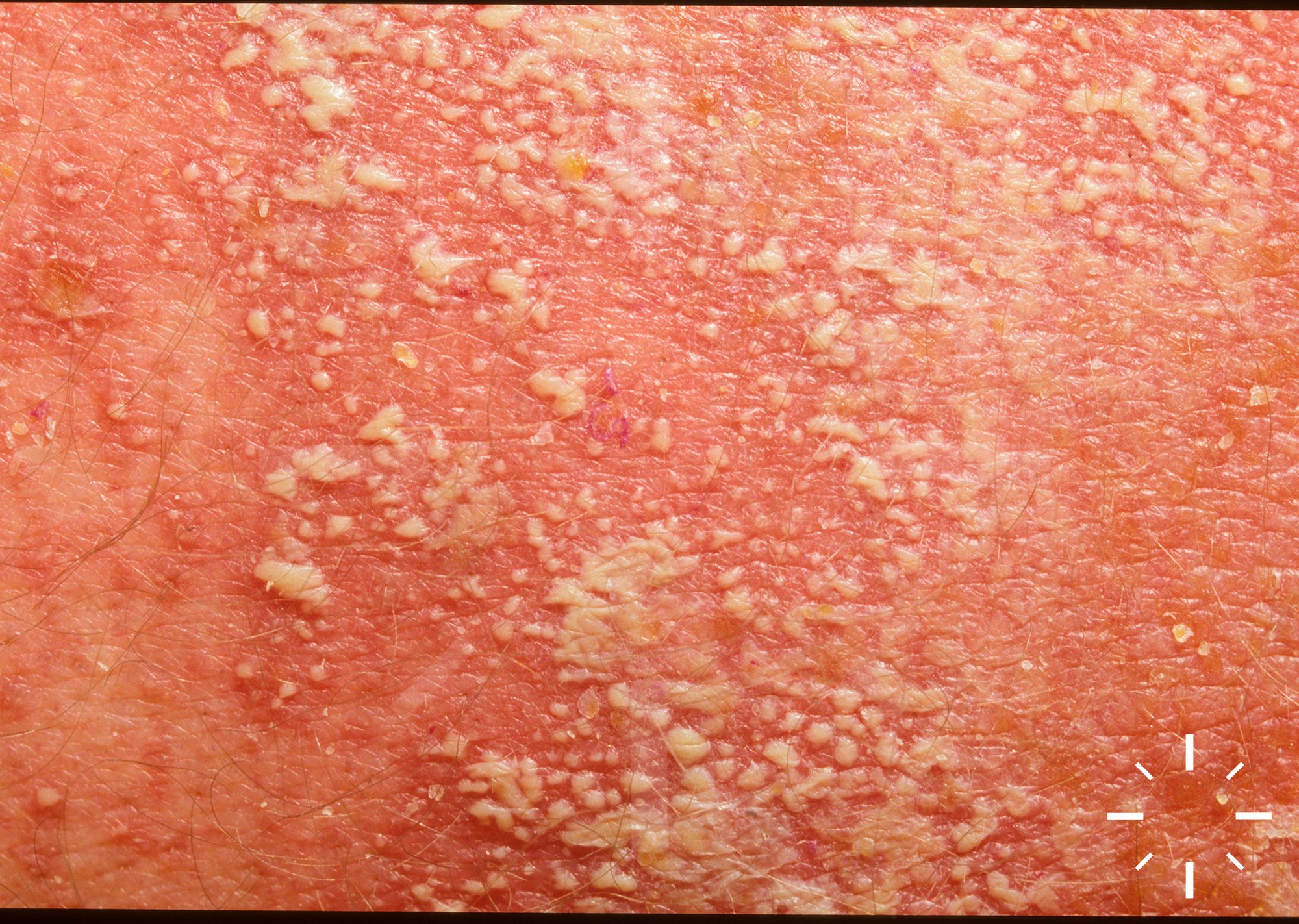
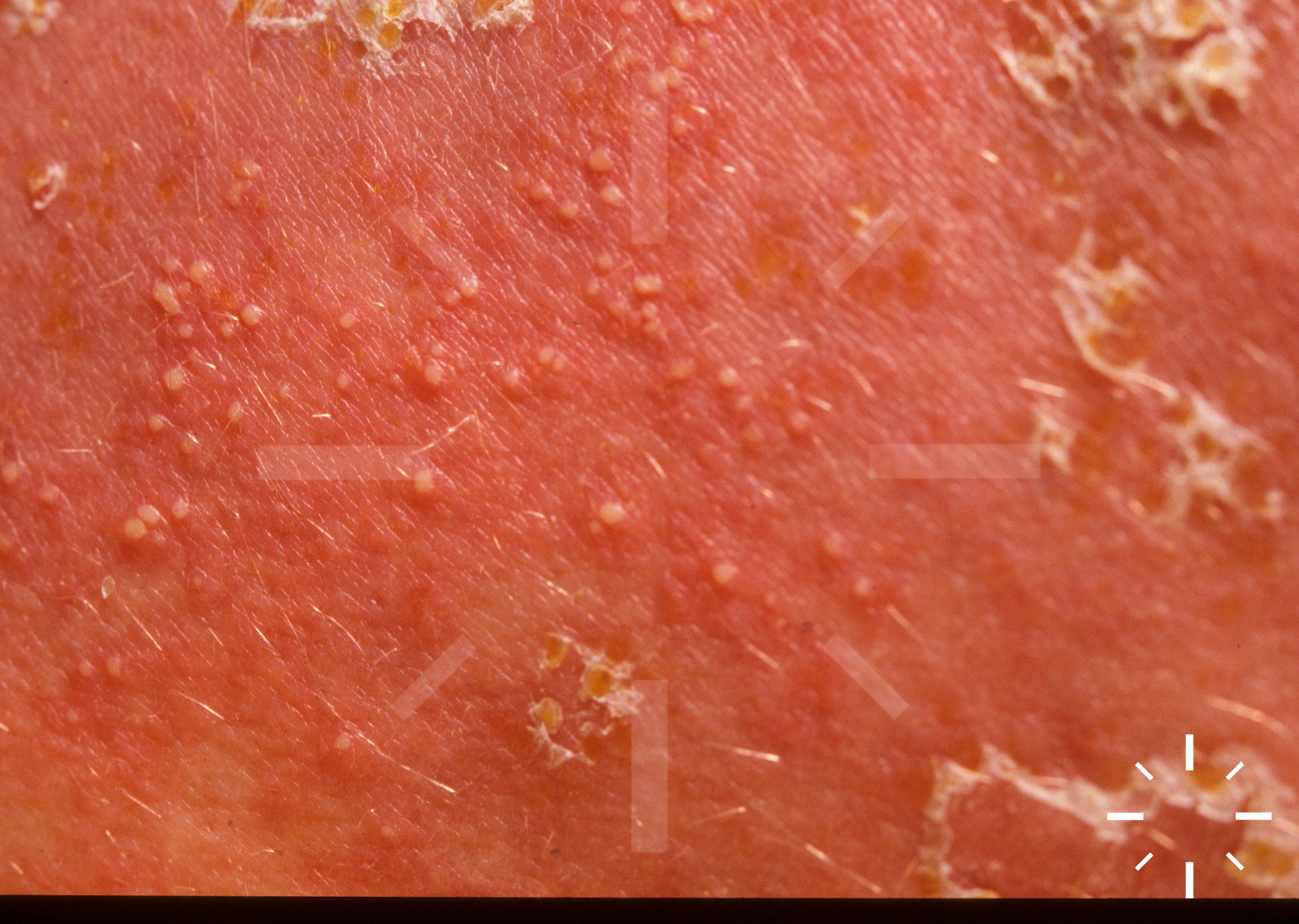
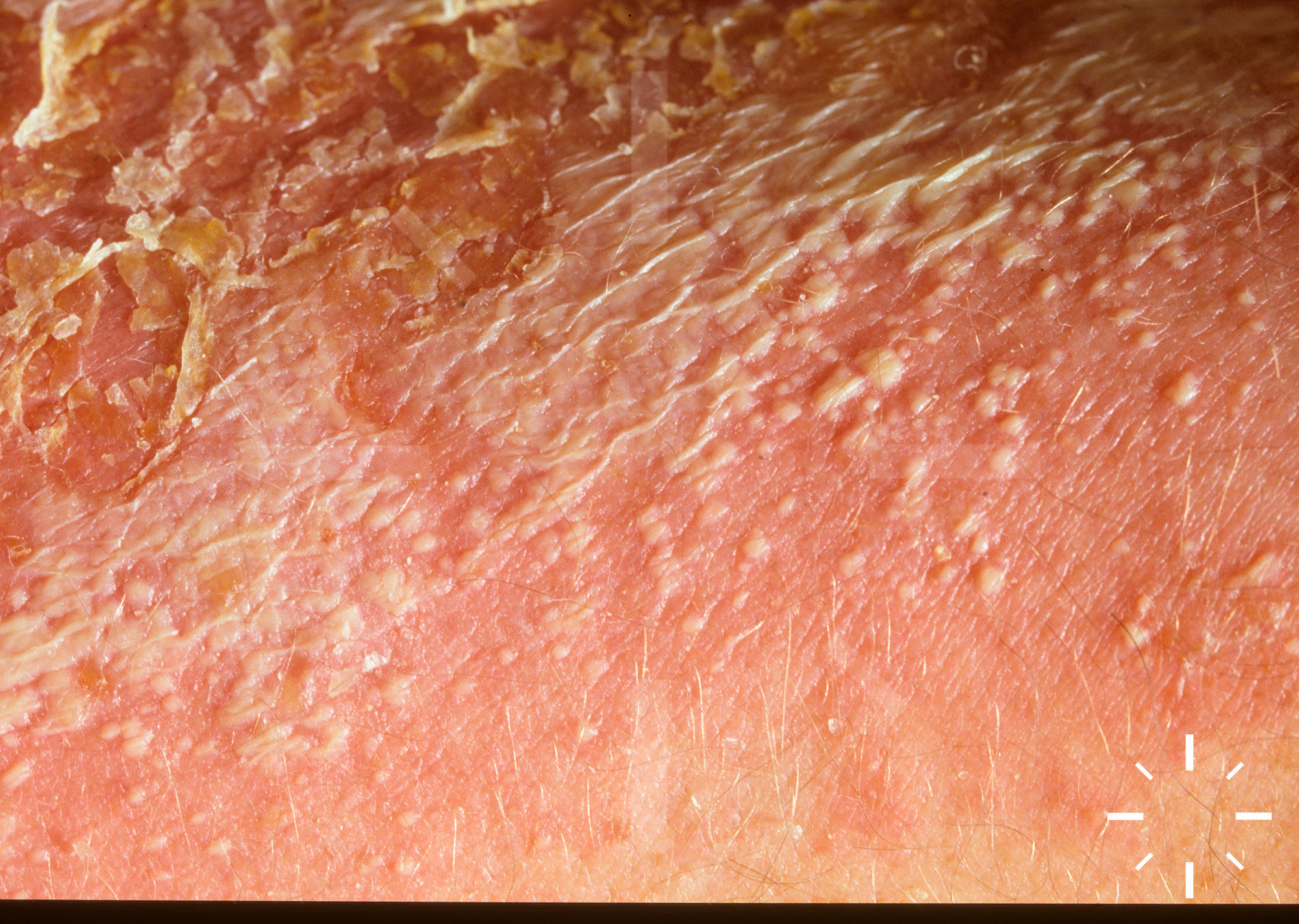
Generalised pustular psoriasis (GPP)
Last Updated: 2023-07-07
Author(s): Navarini A.
ICD11: EA90.40

















1/25