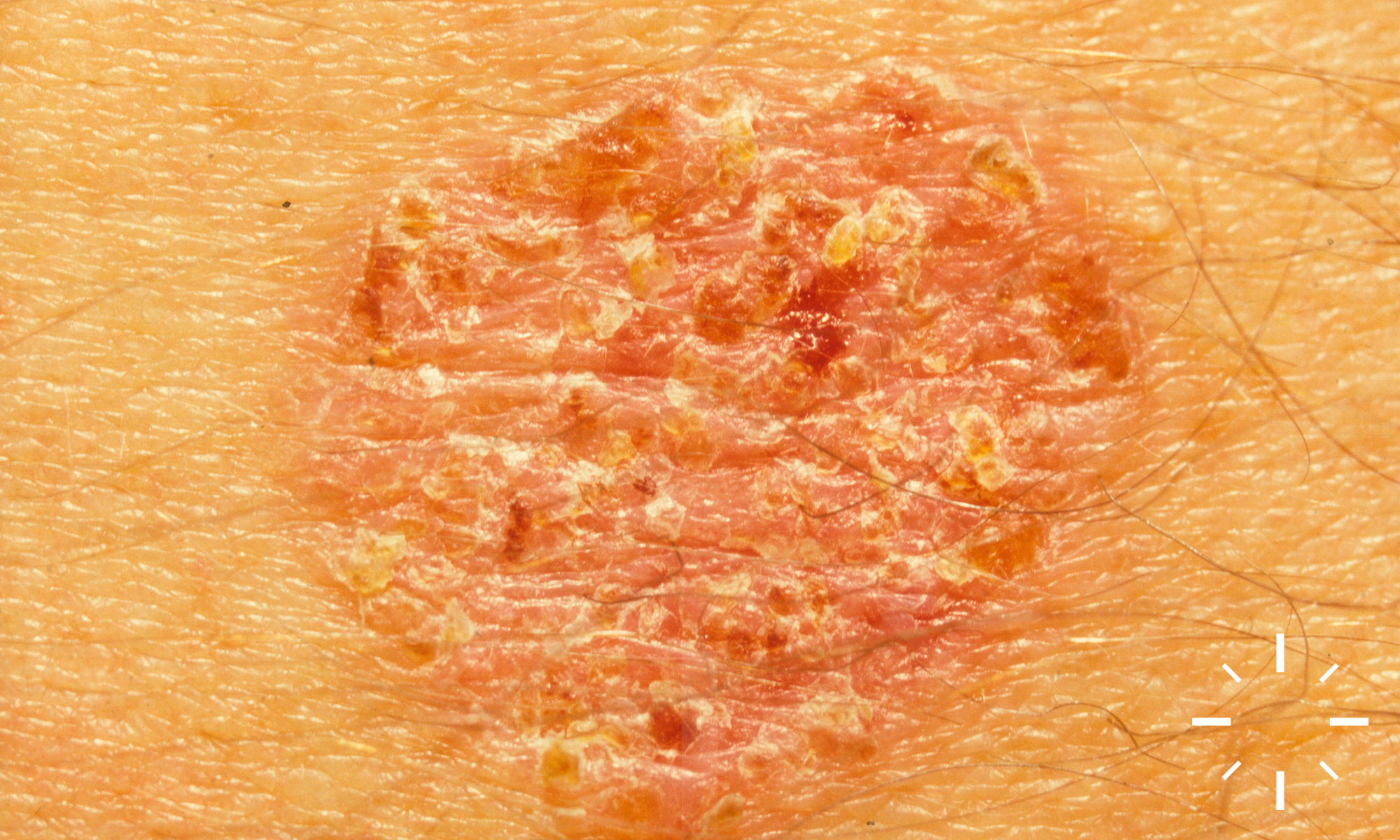
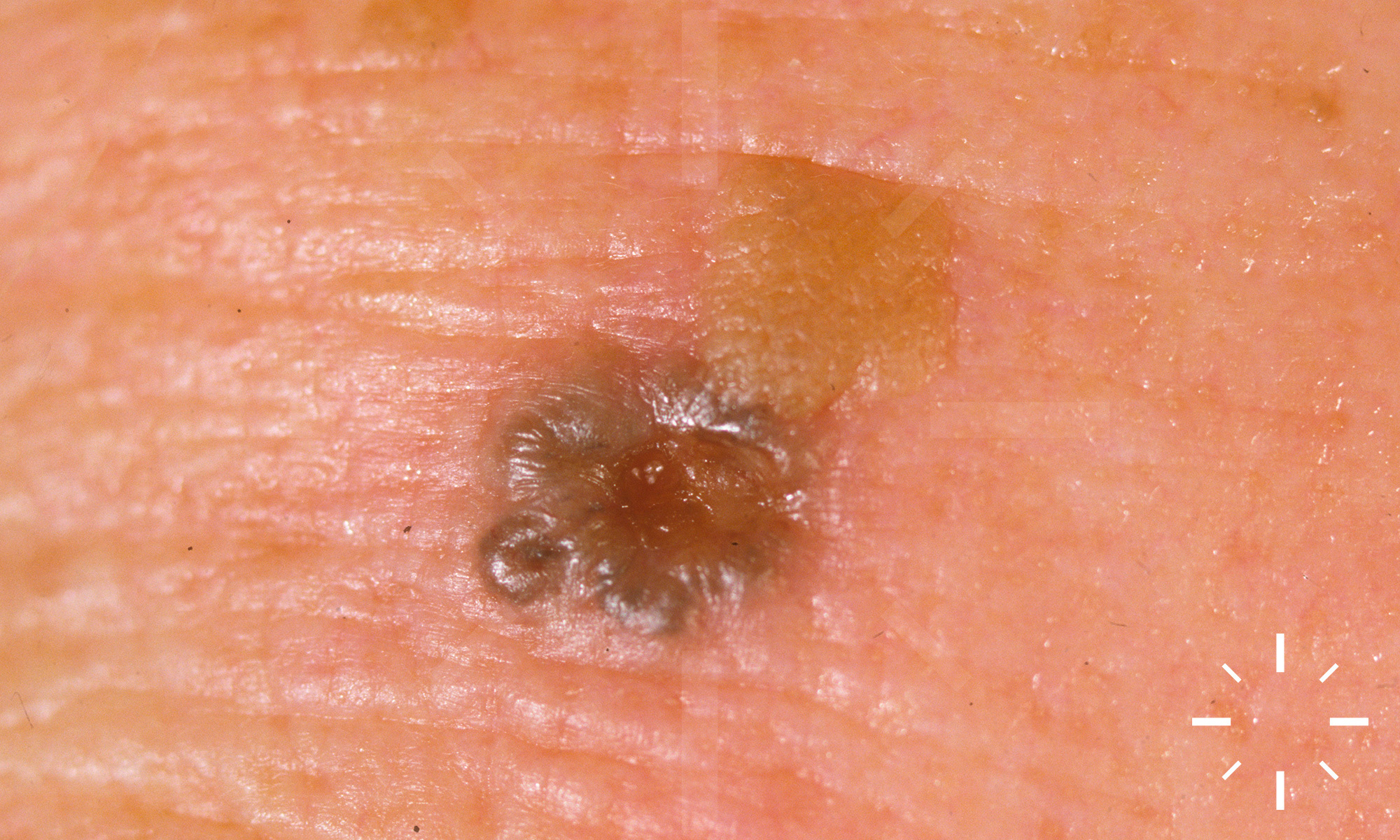
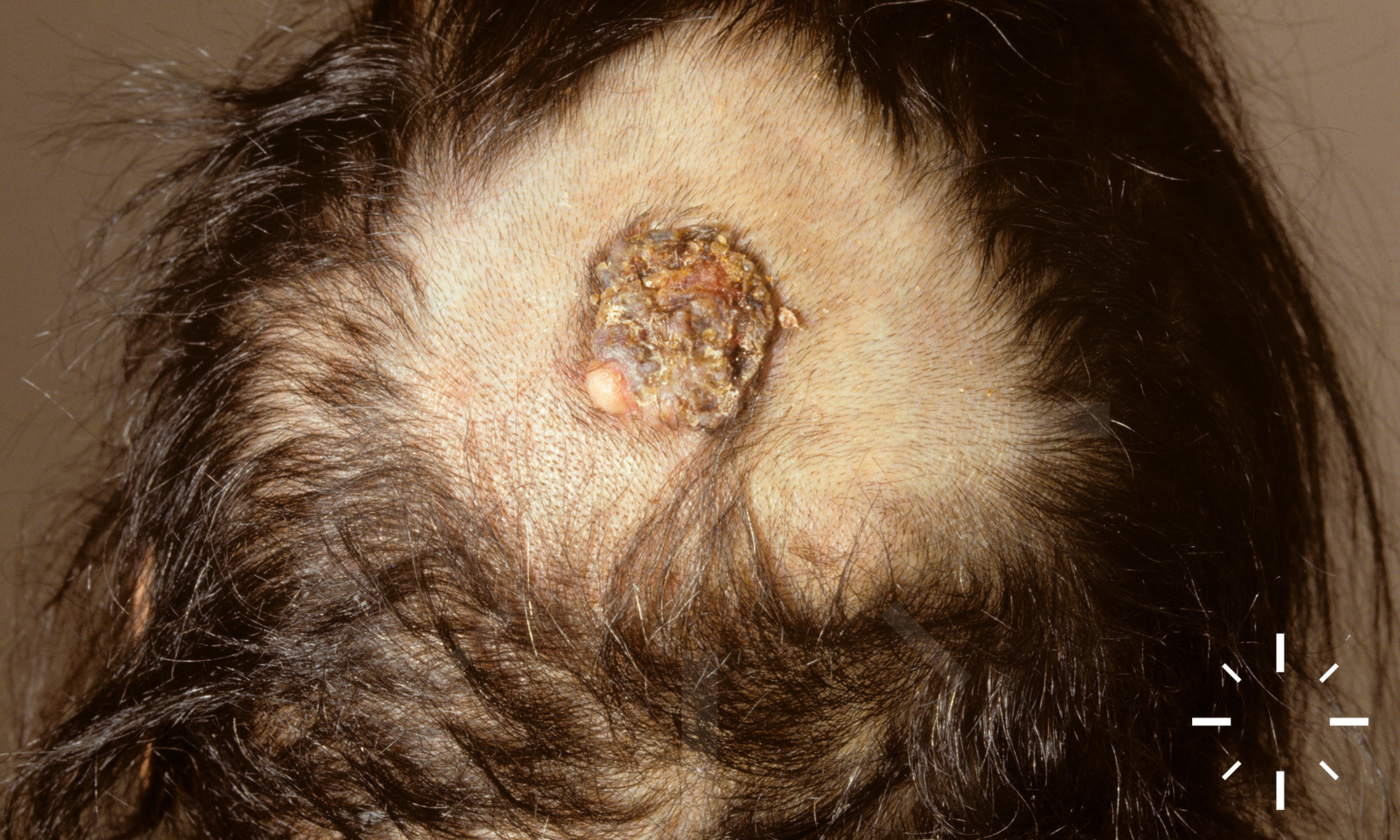
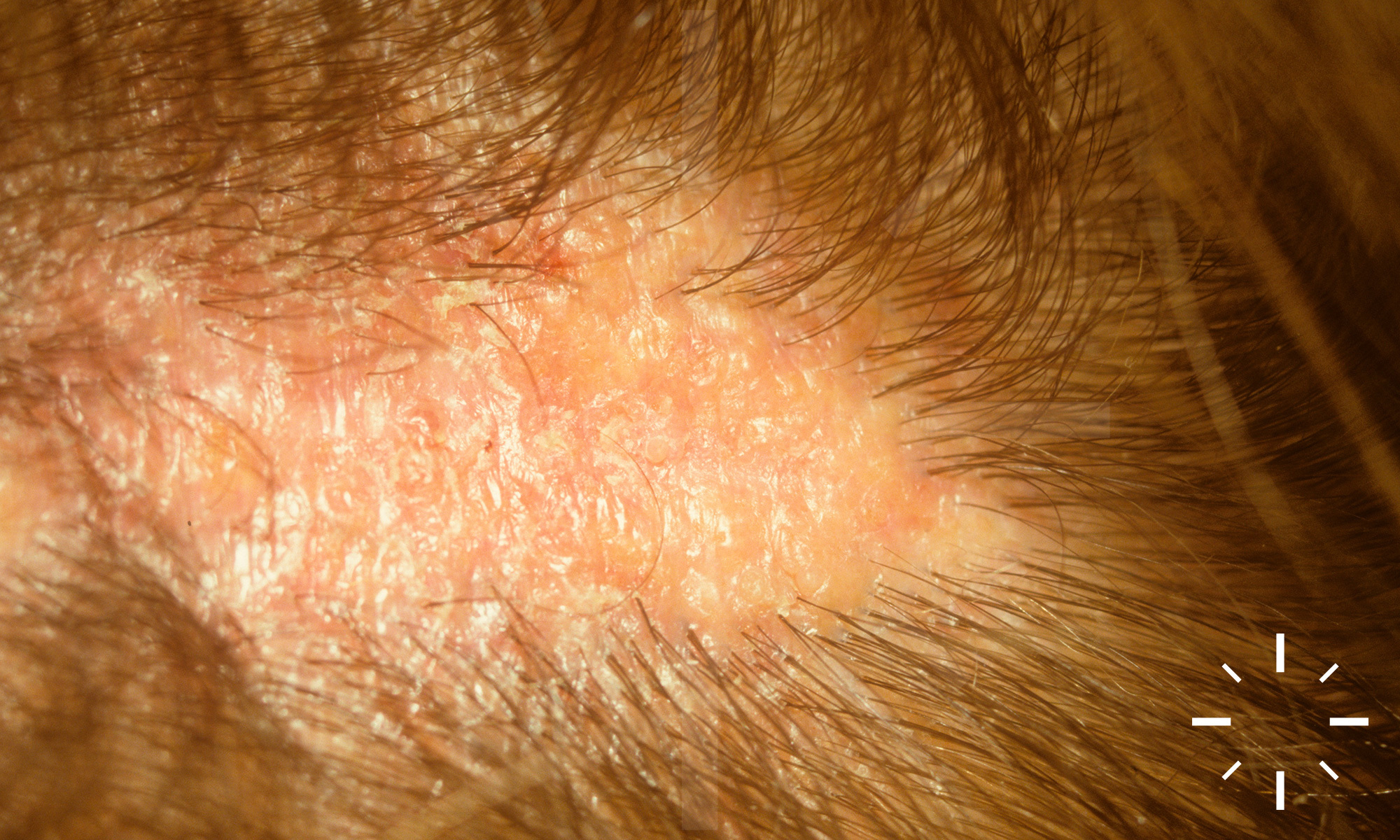
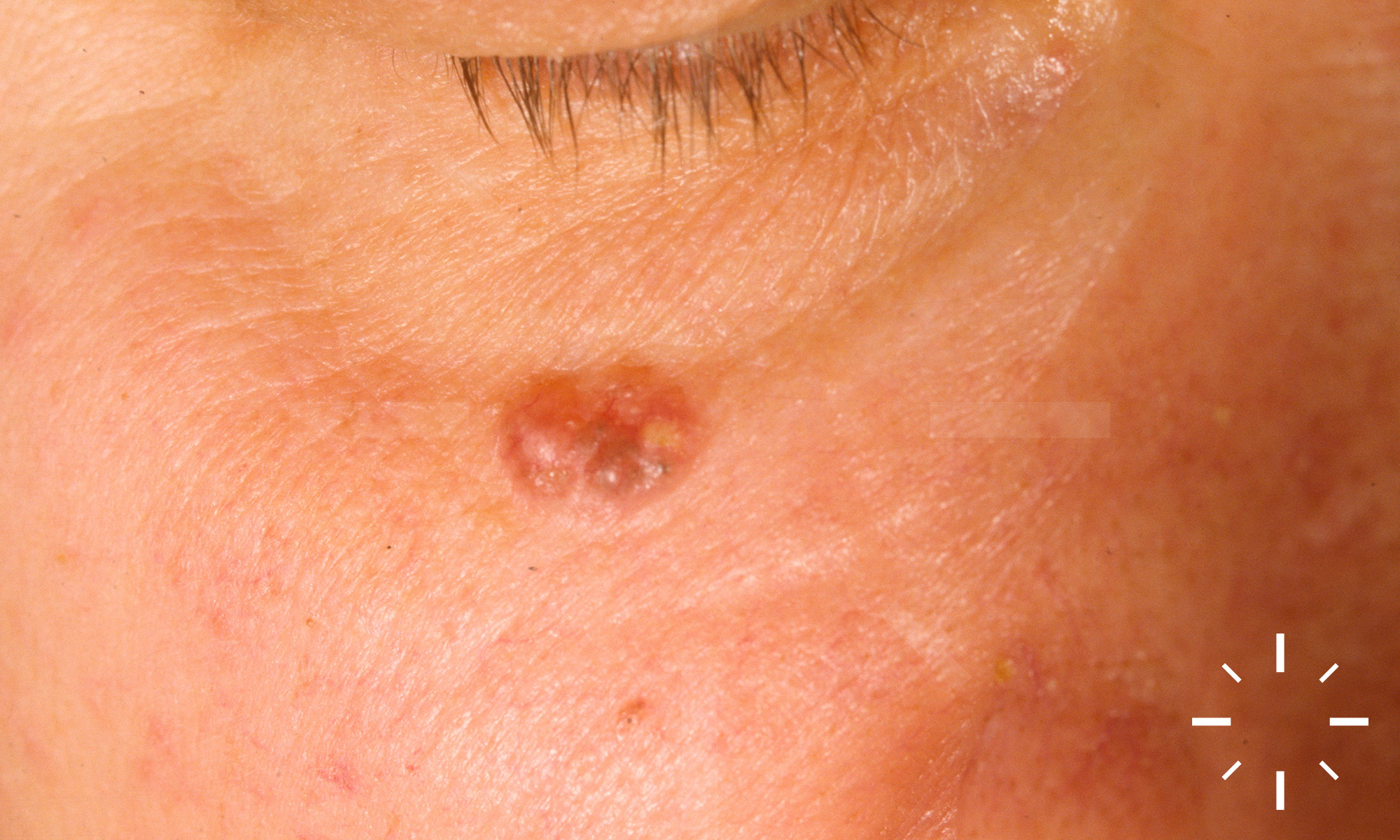
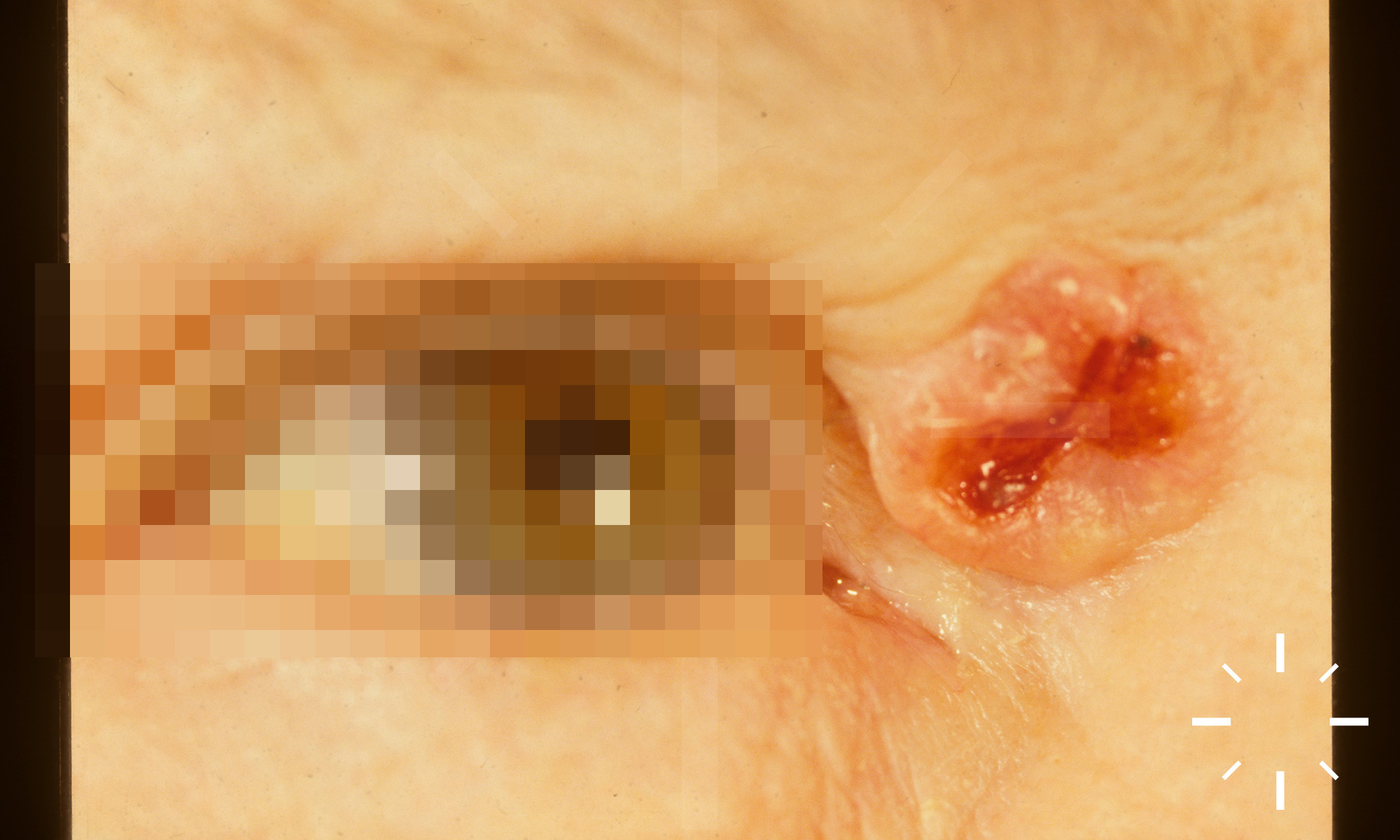
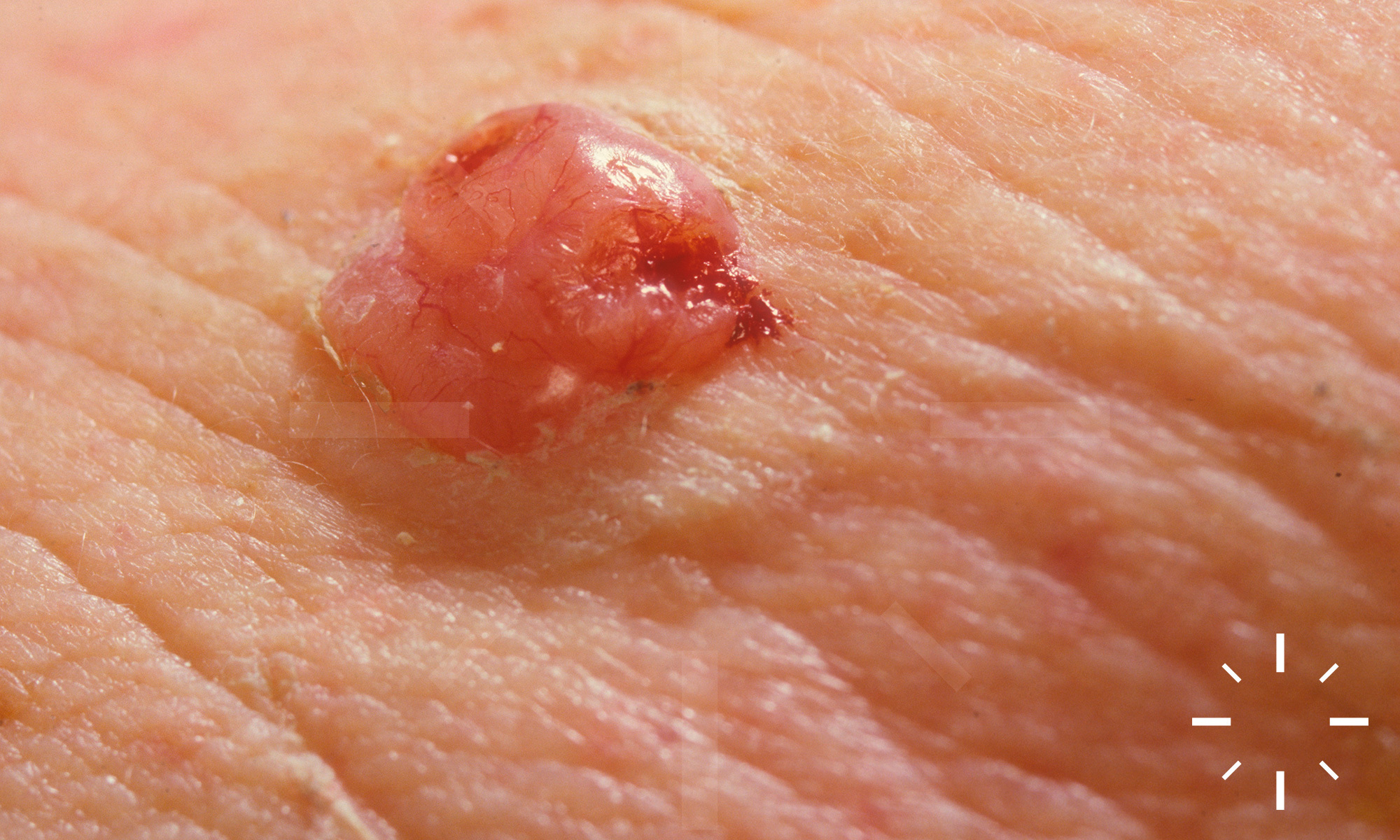
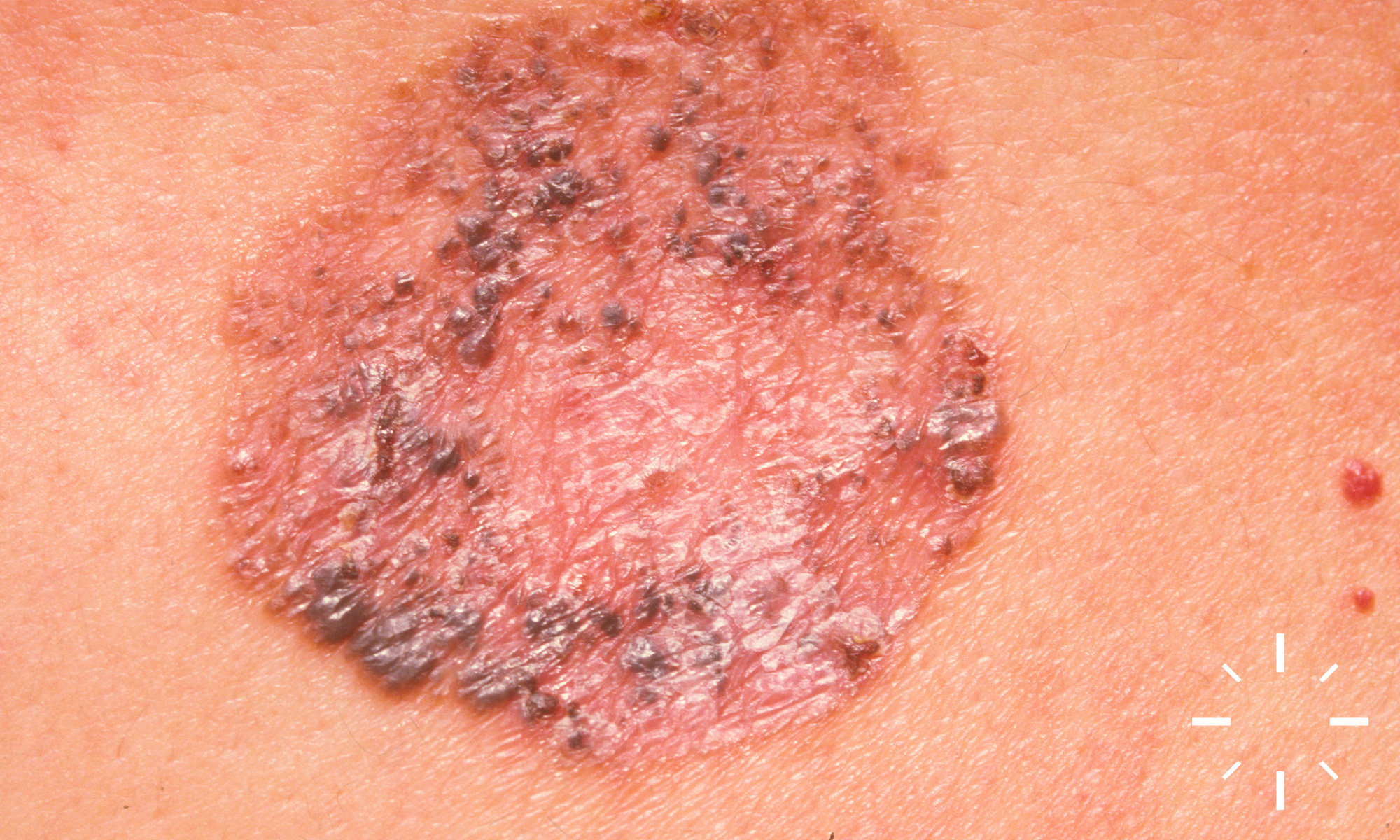
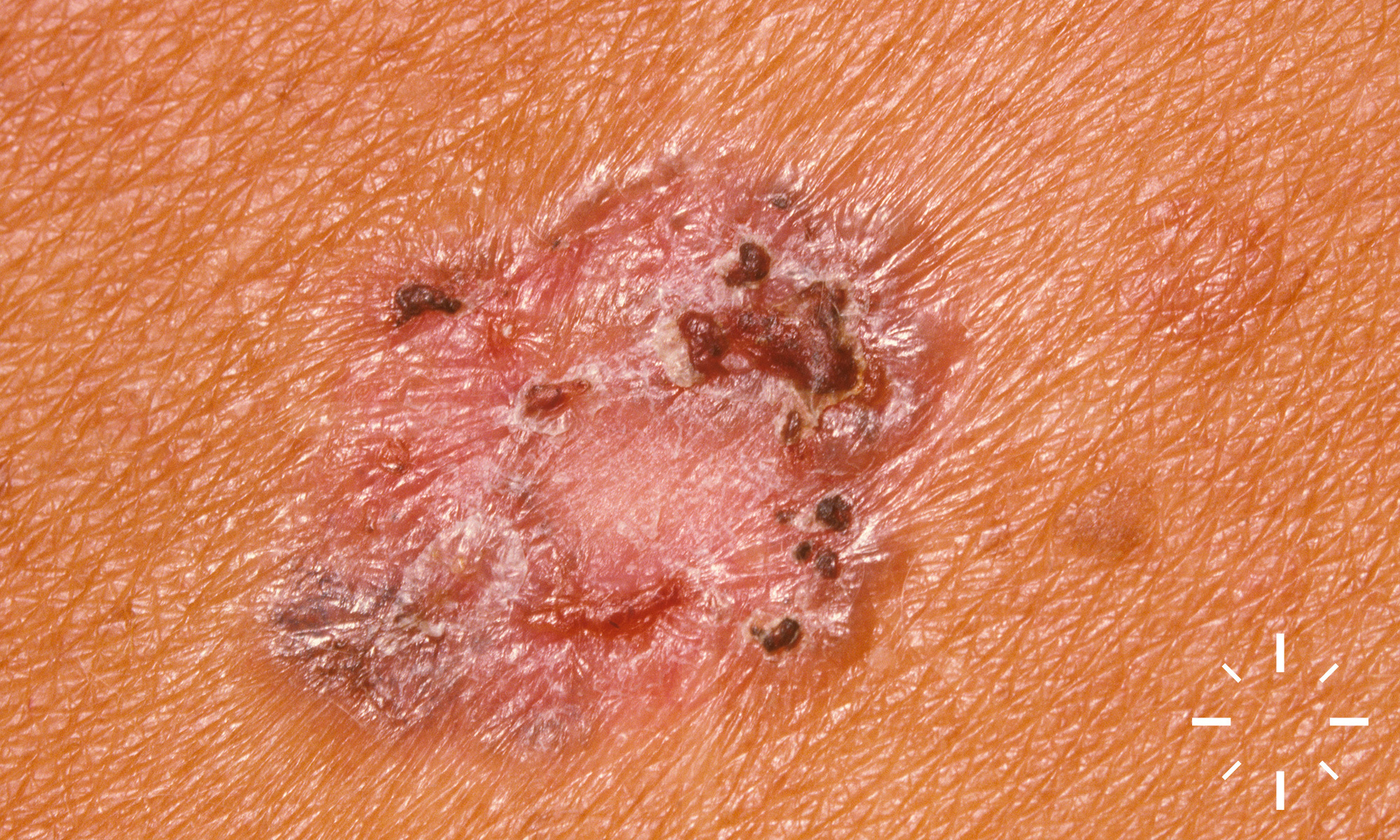
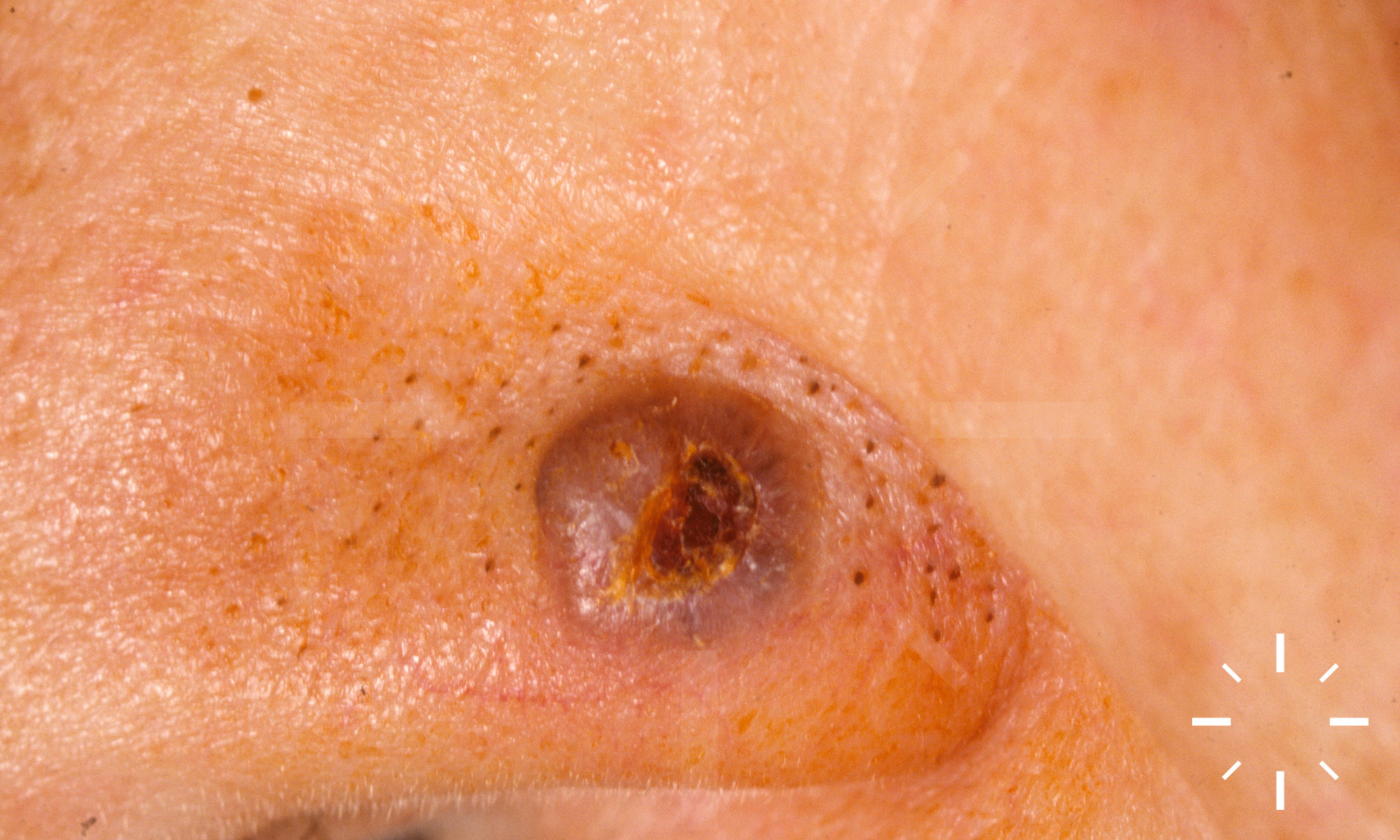
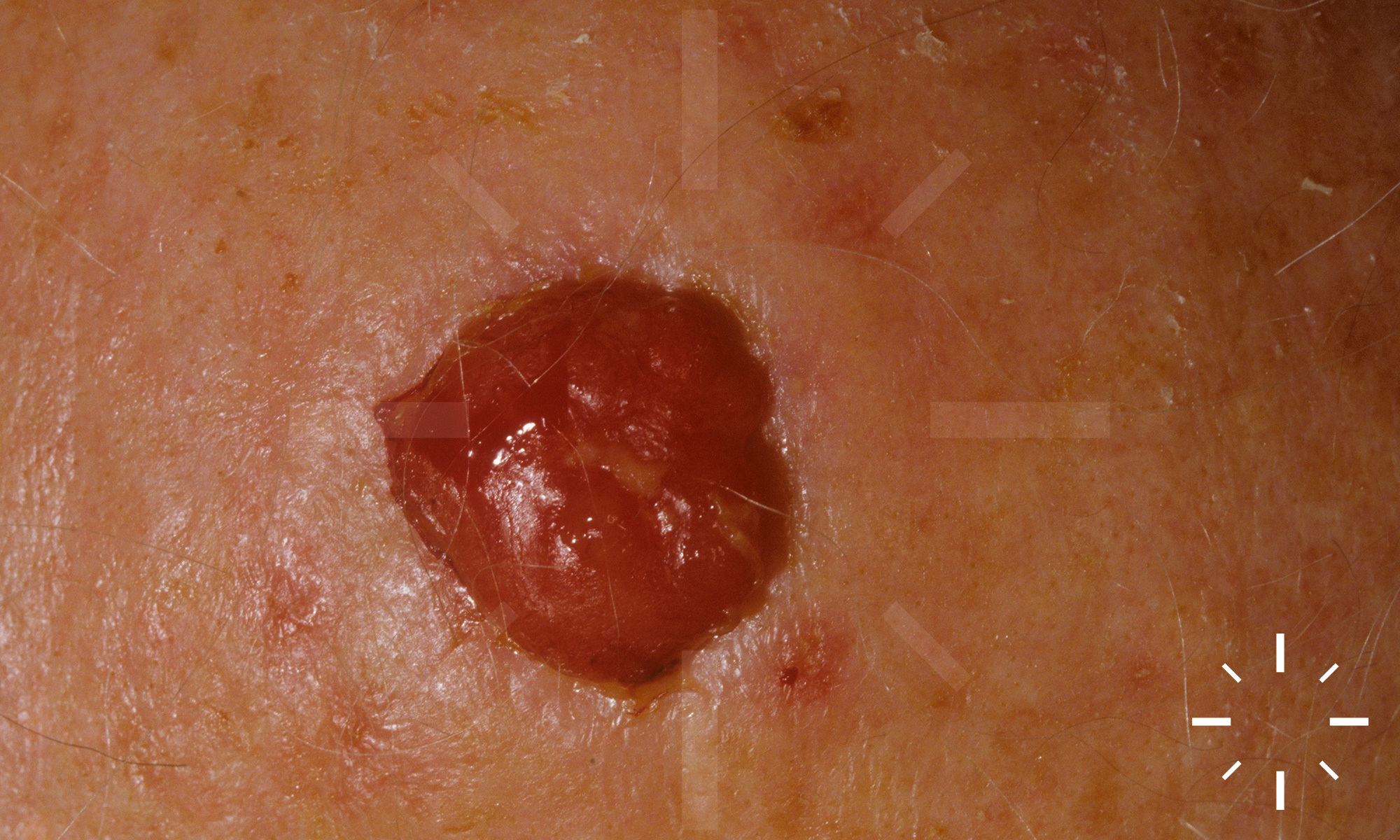
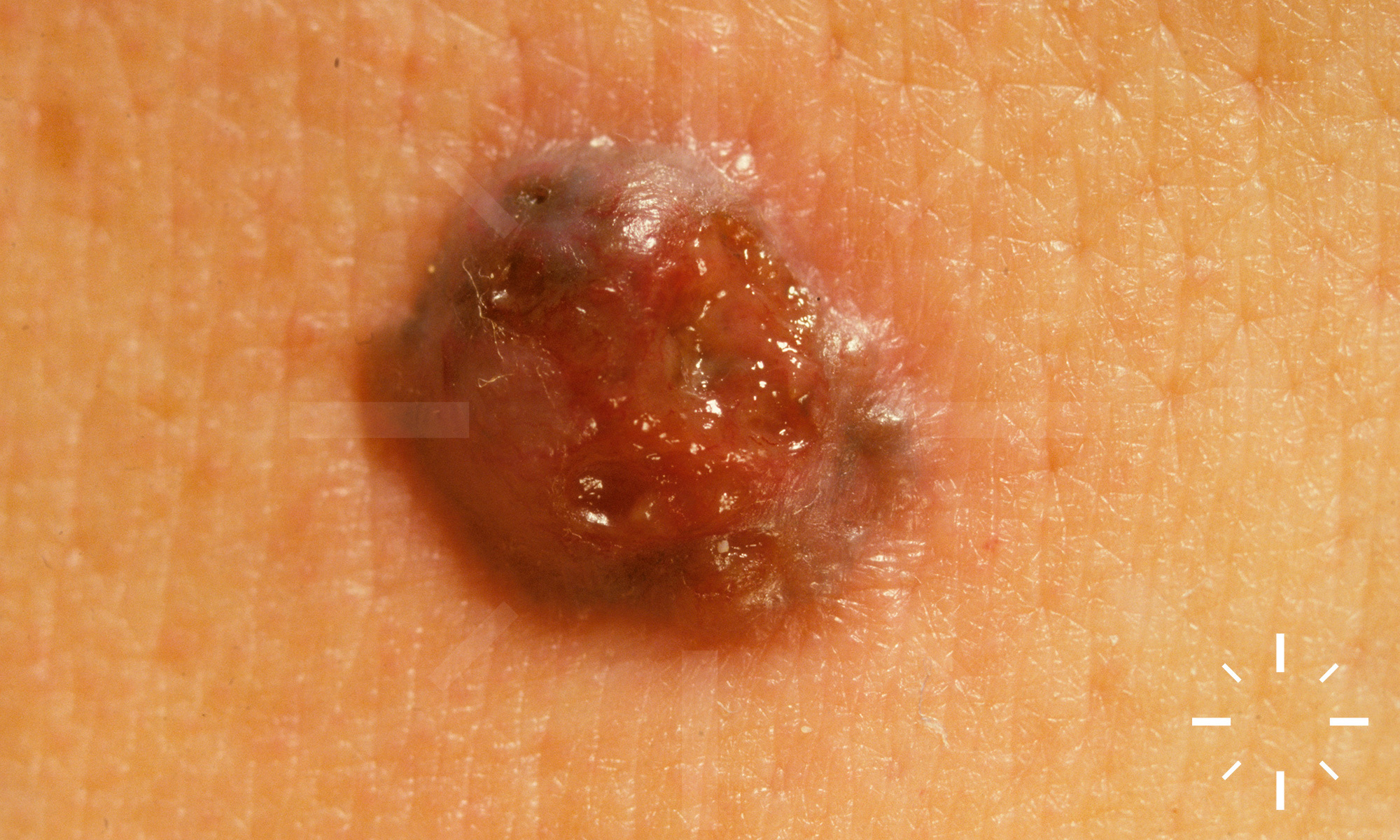
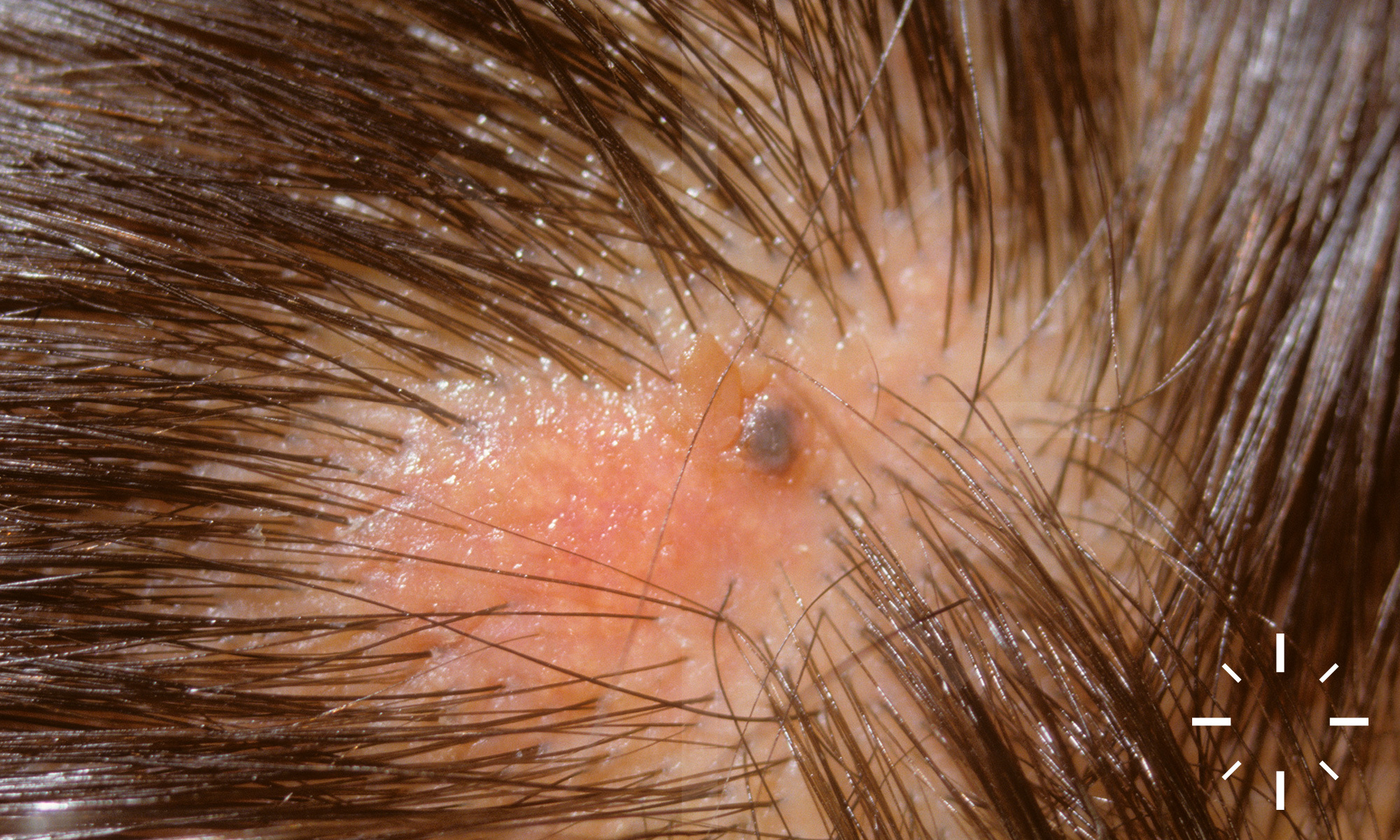
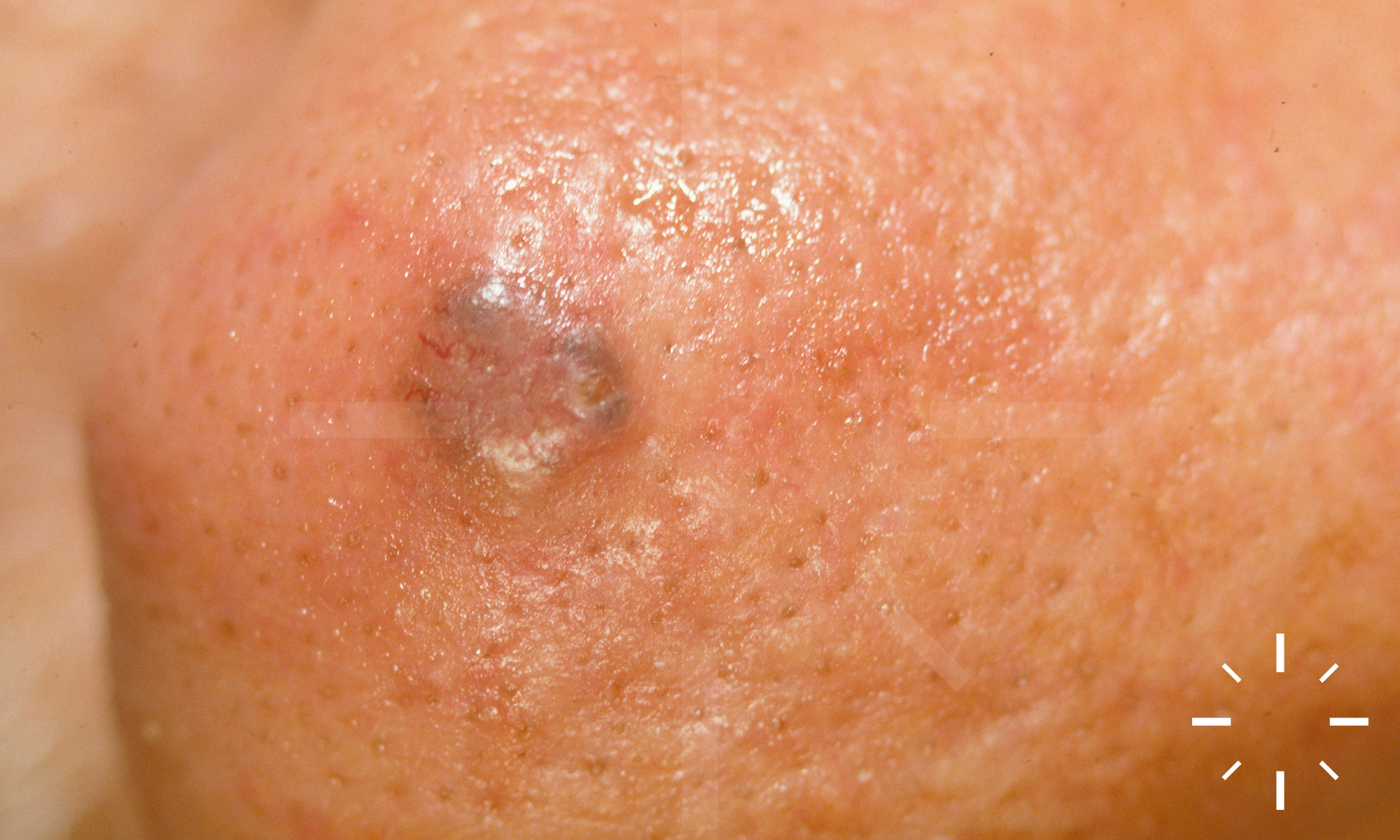
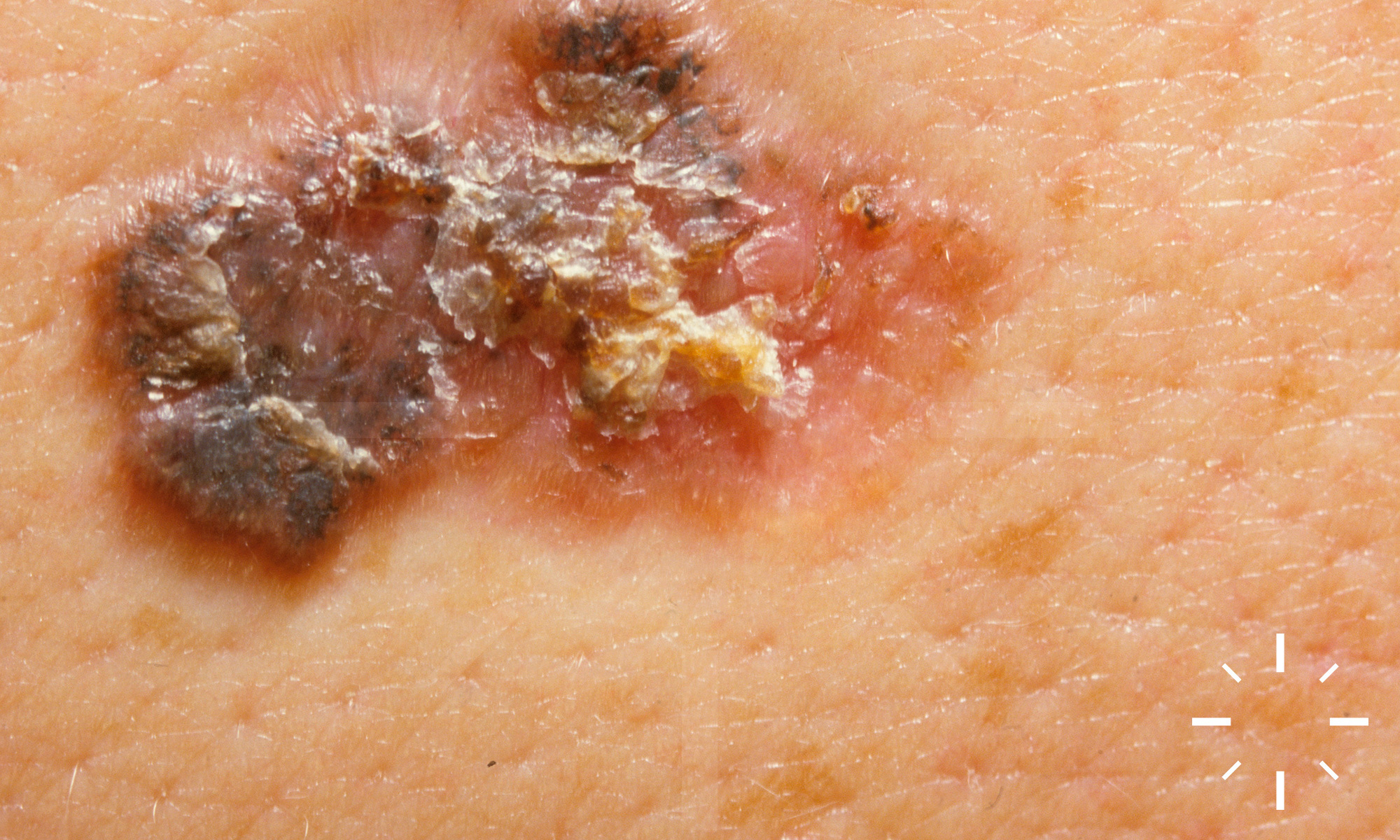
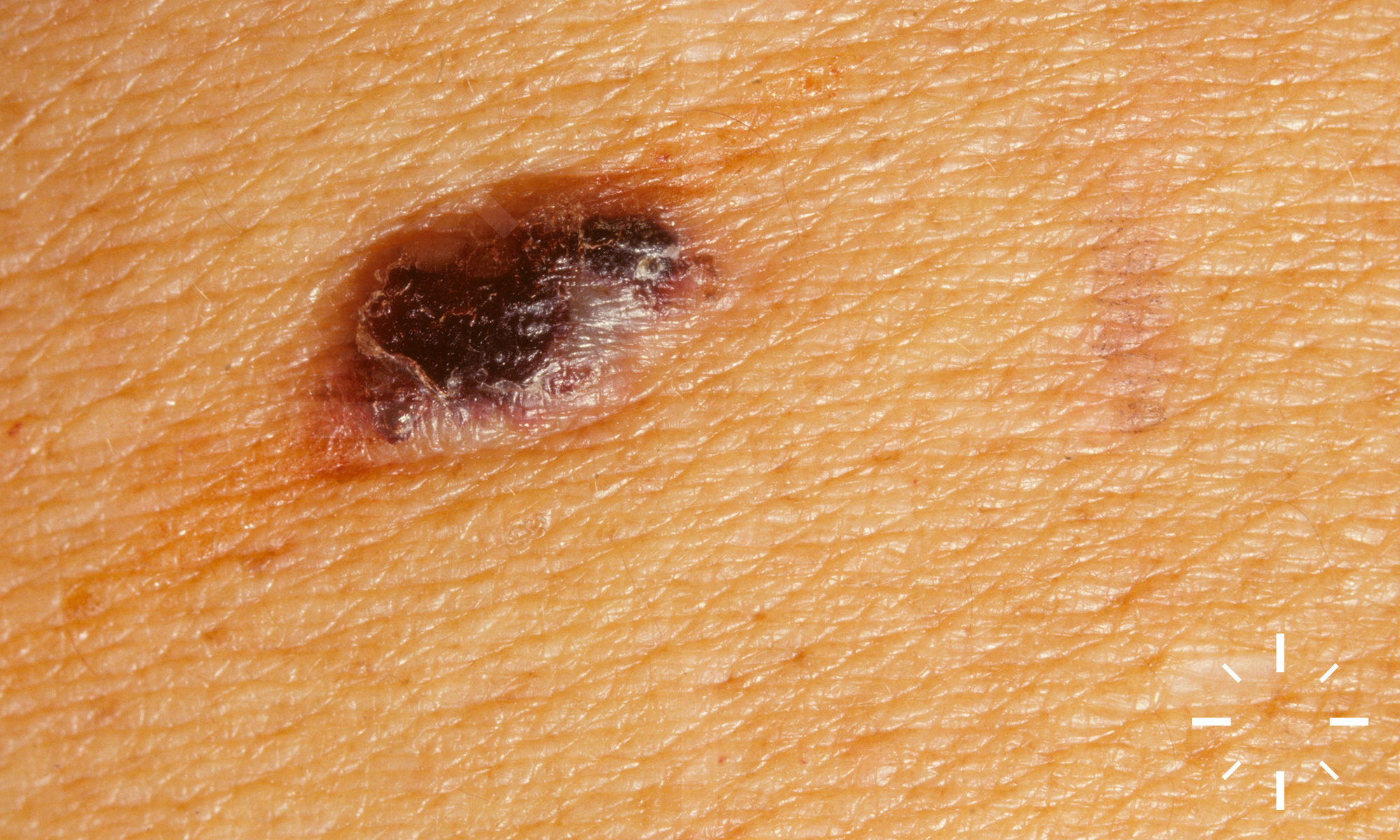
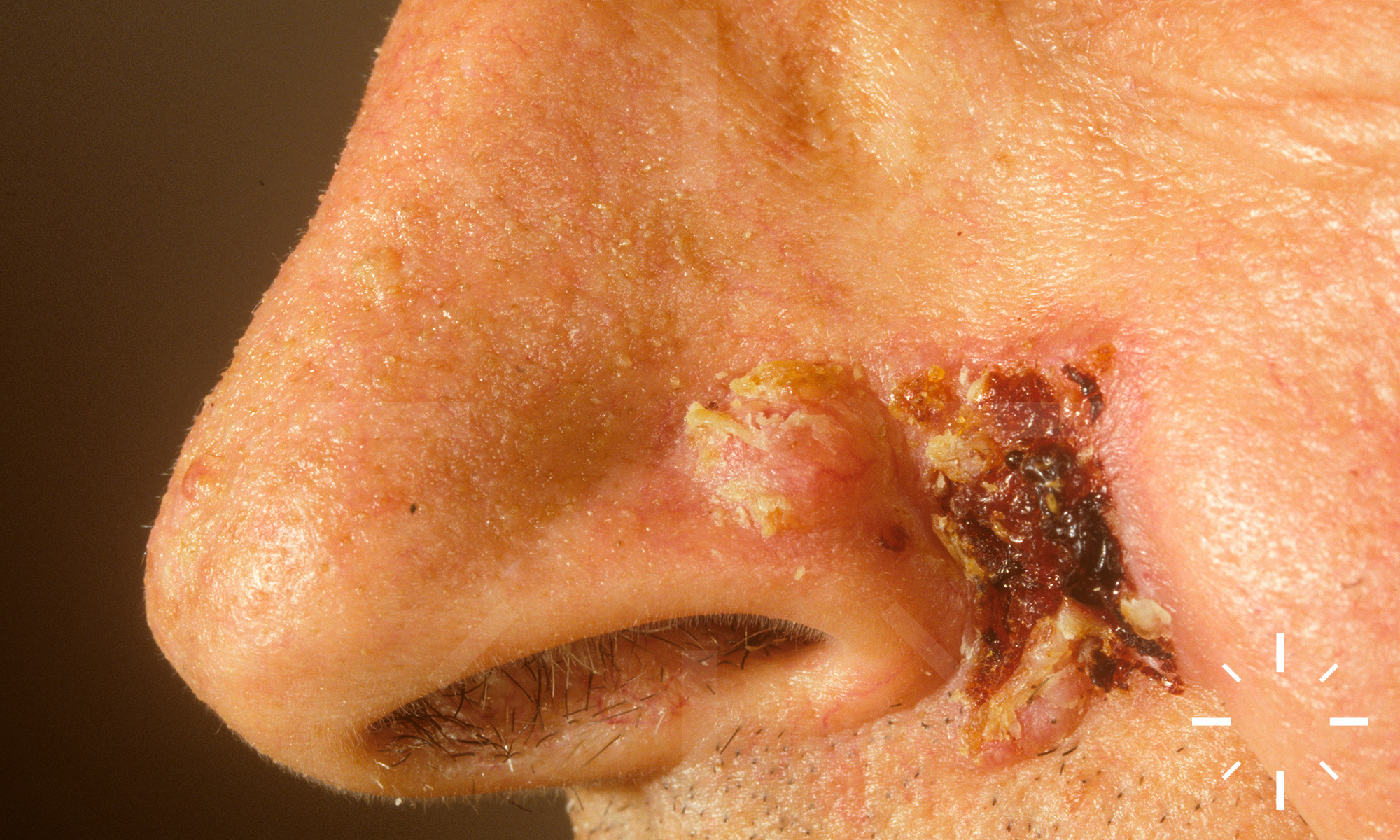
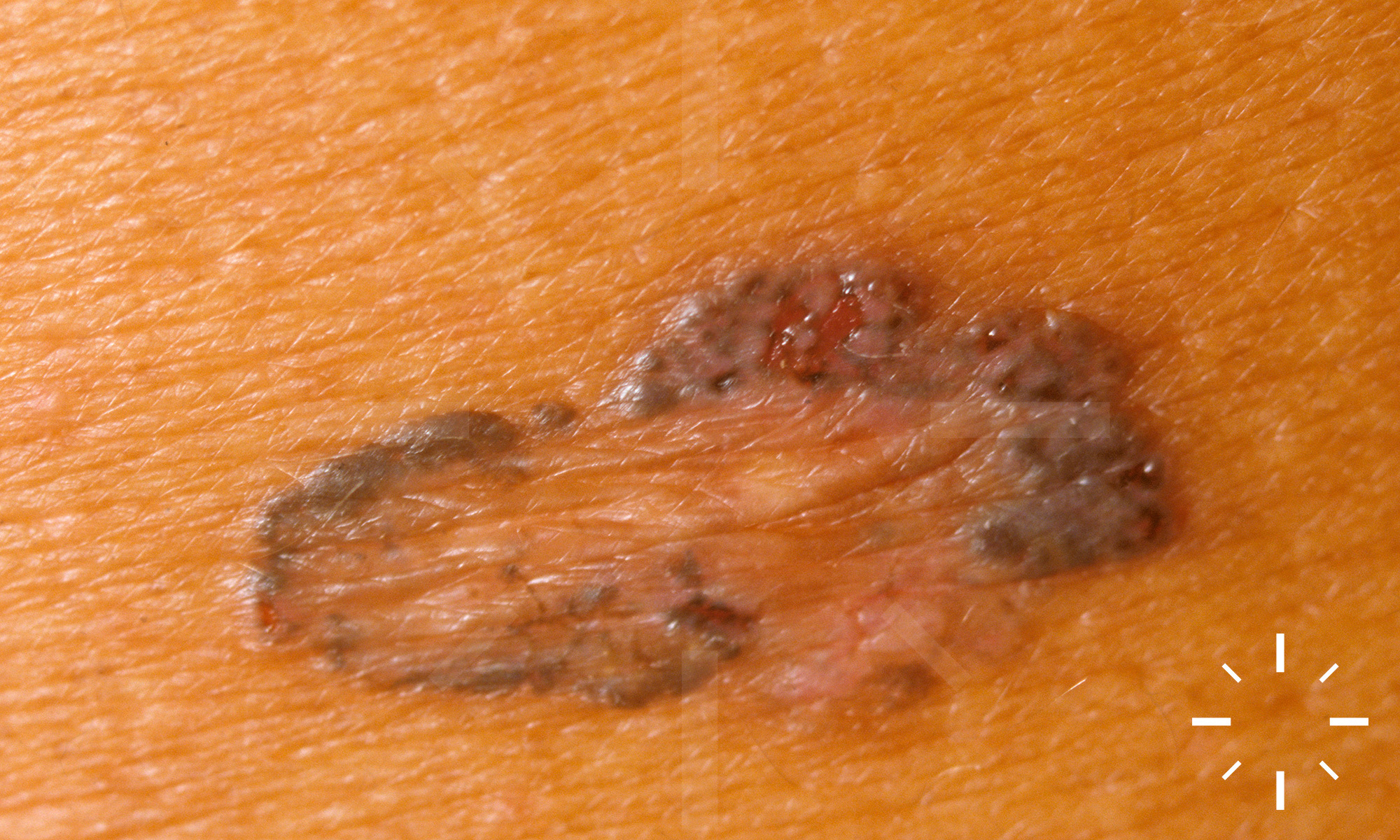
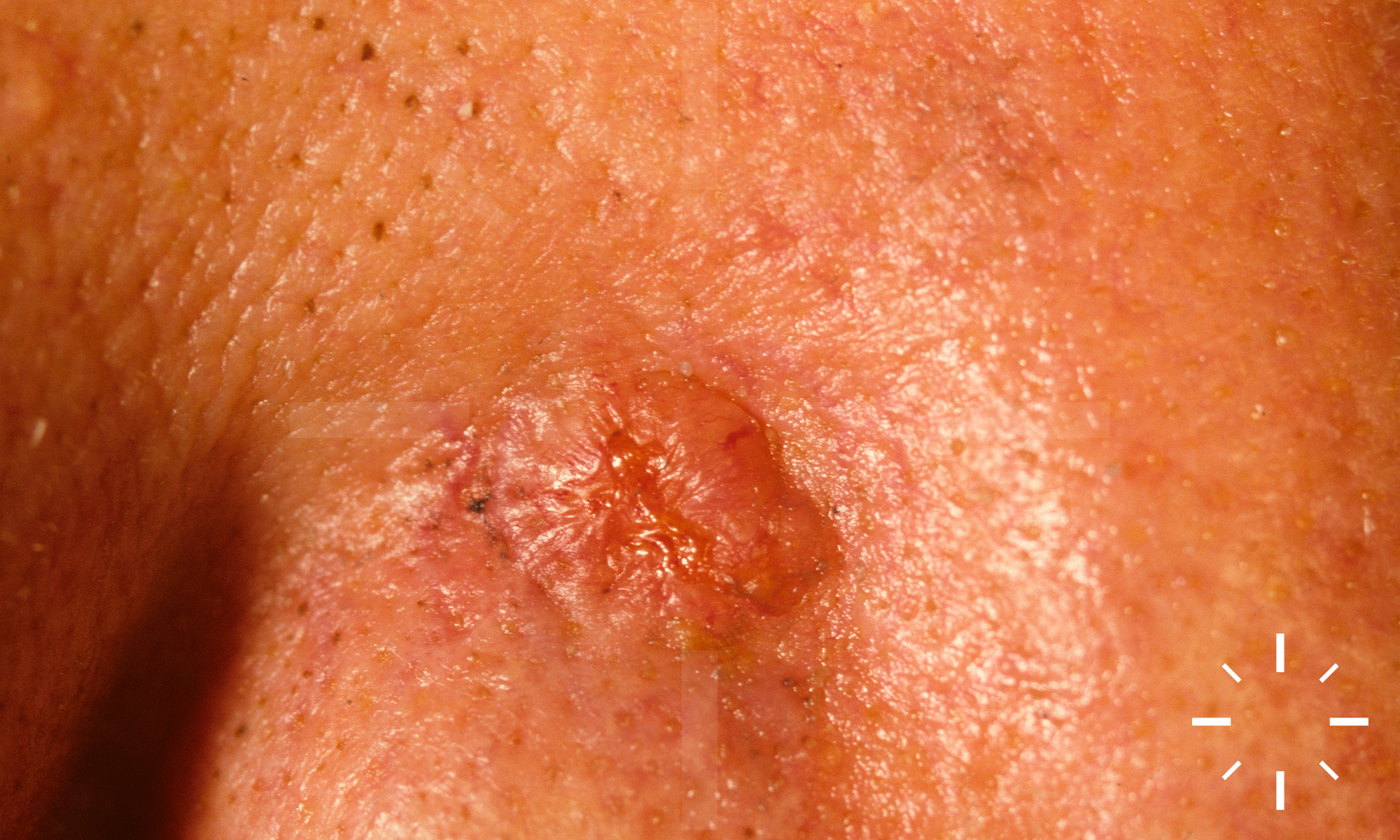
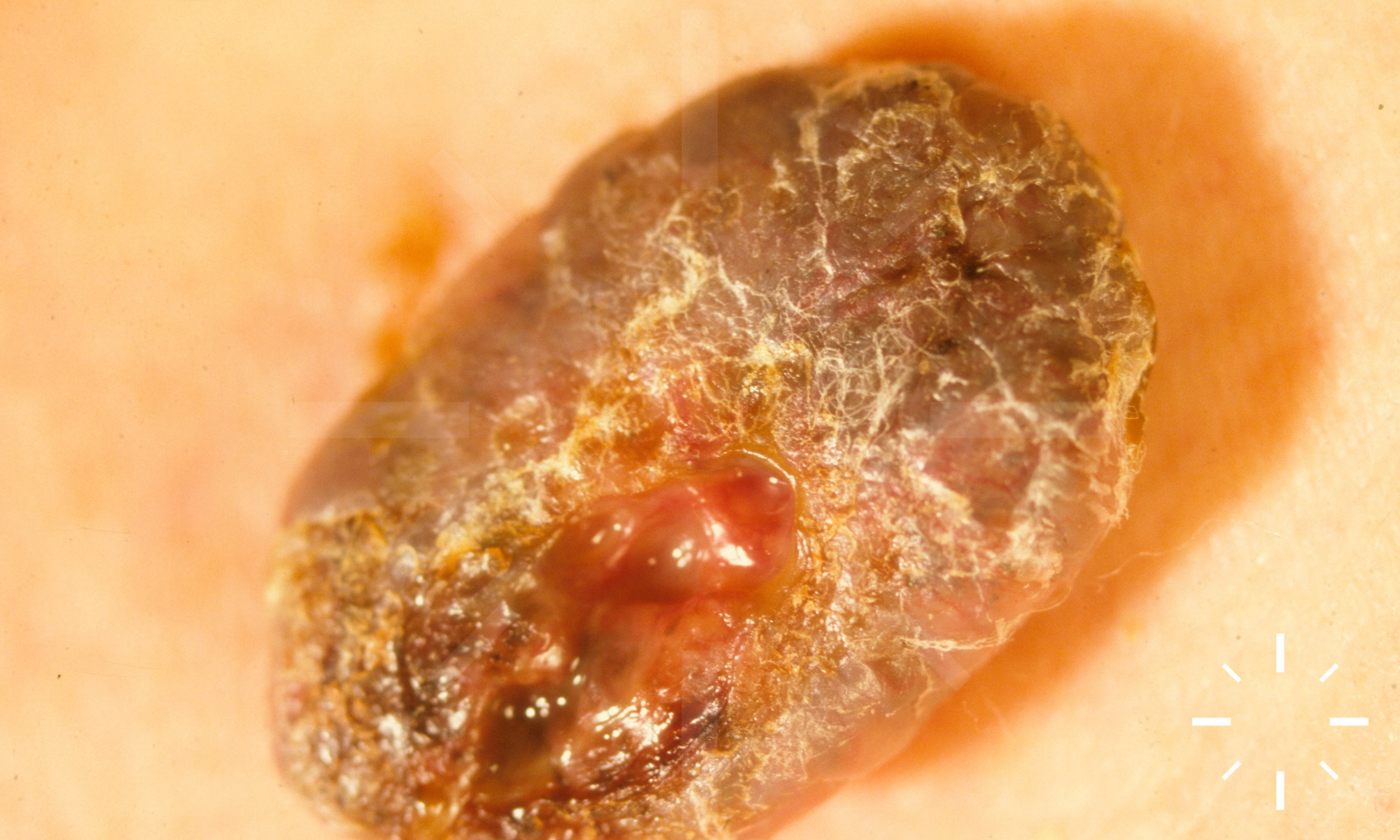
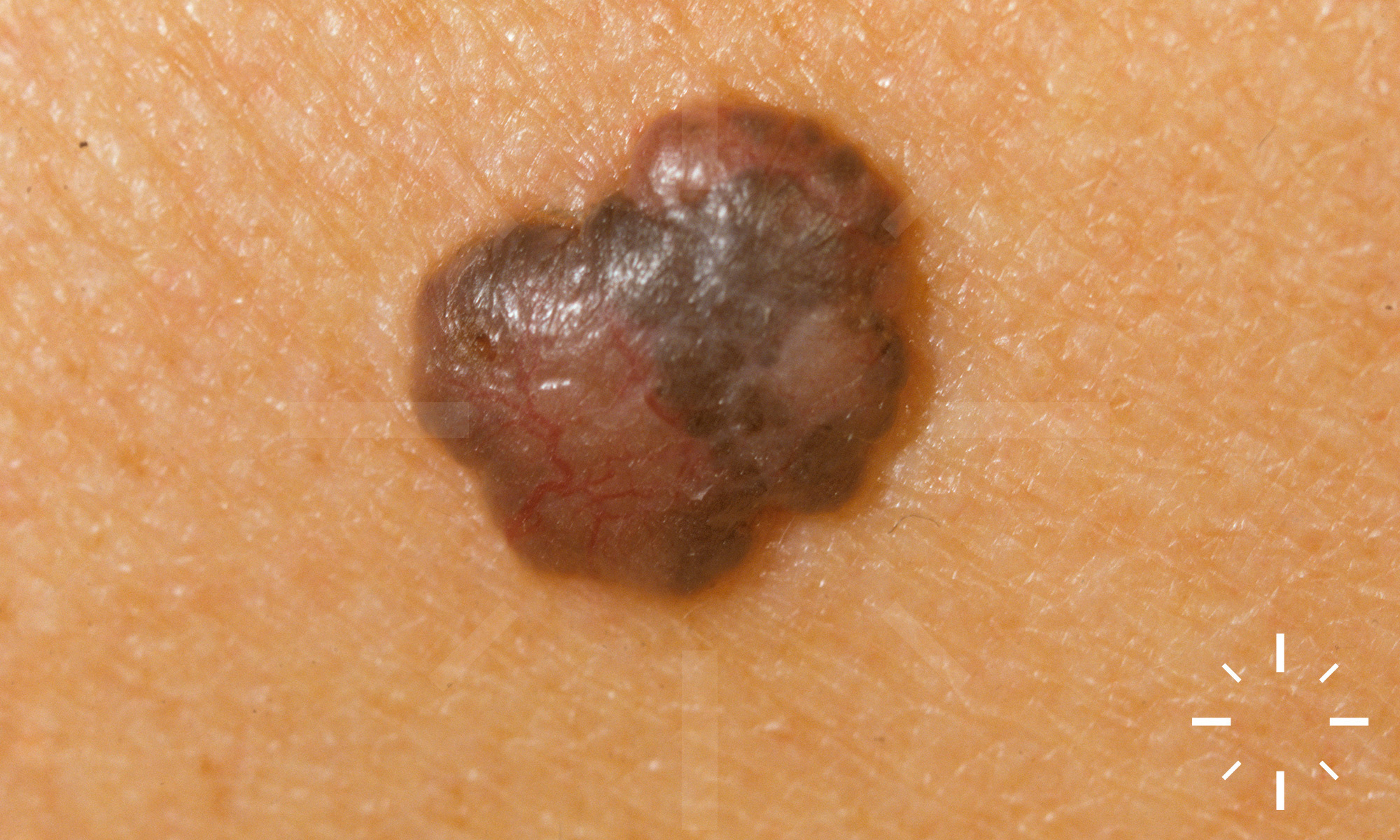
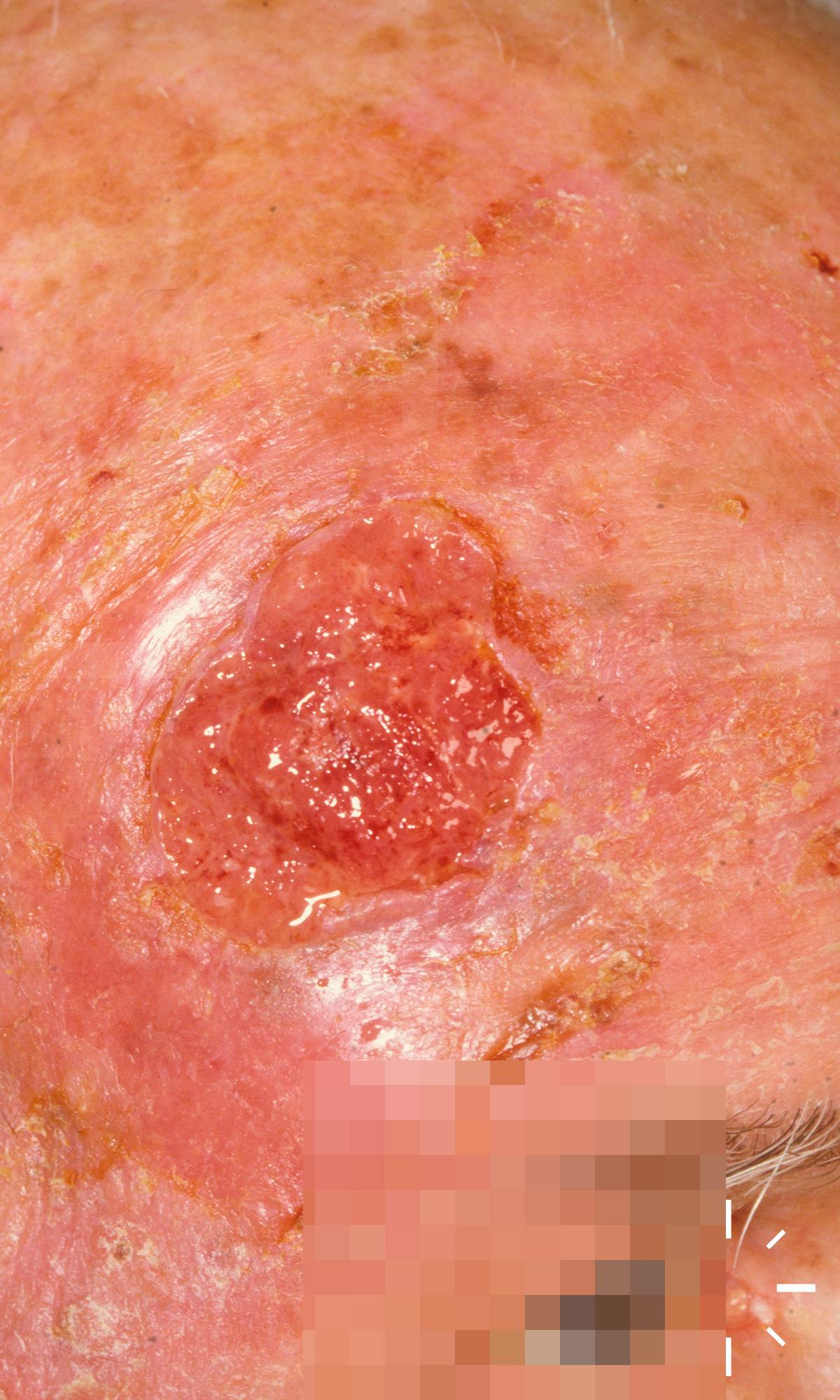
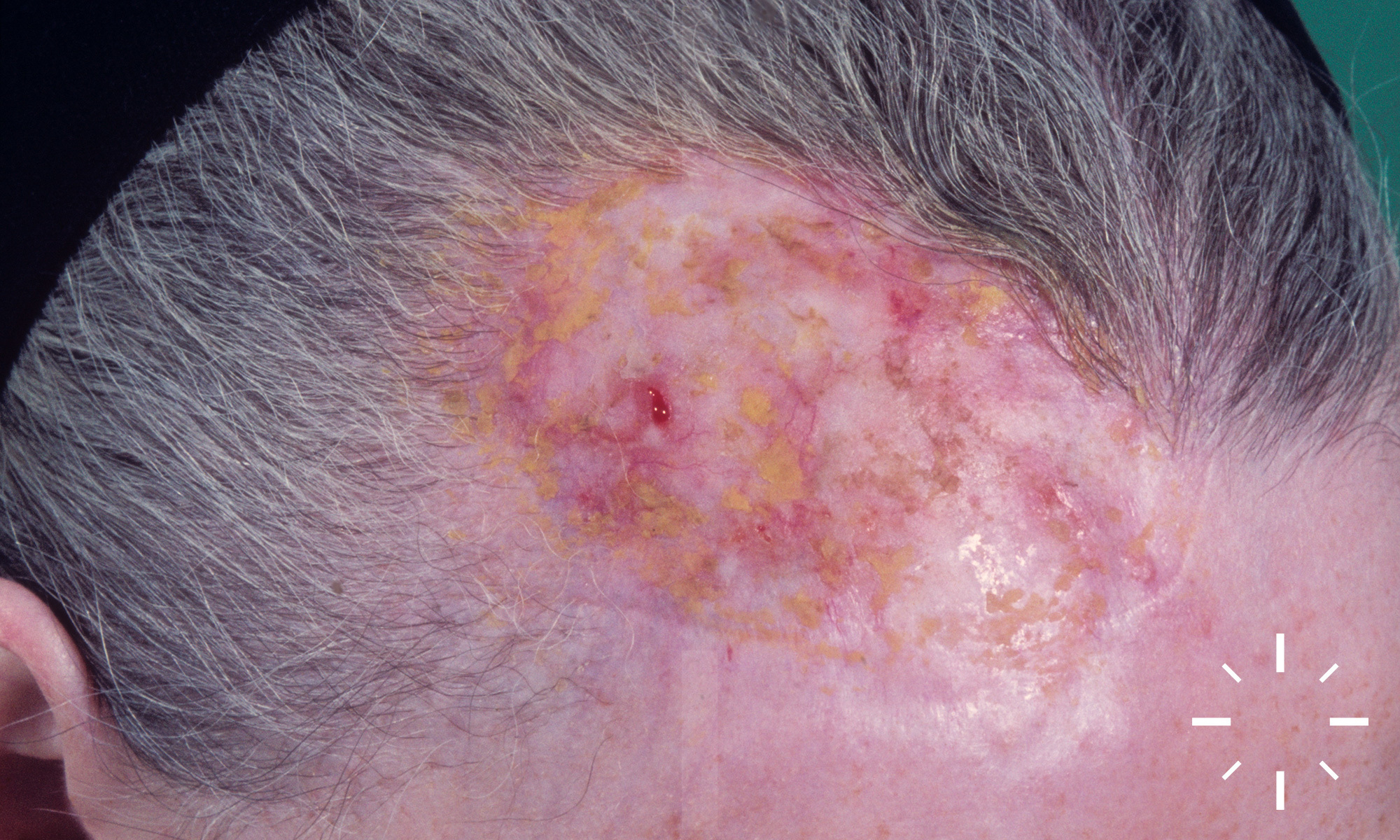
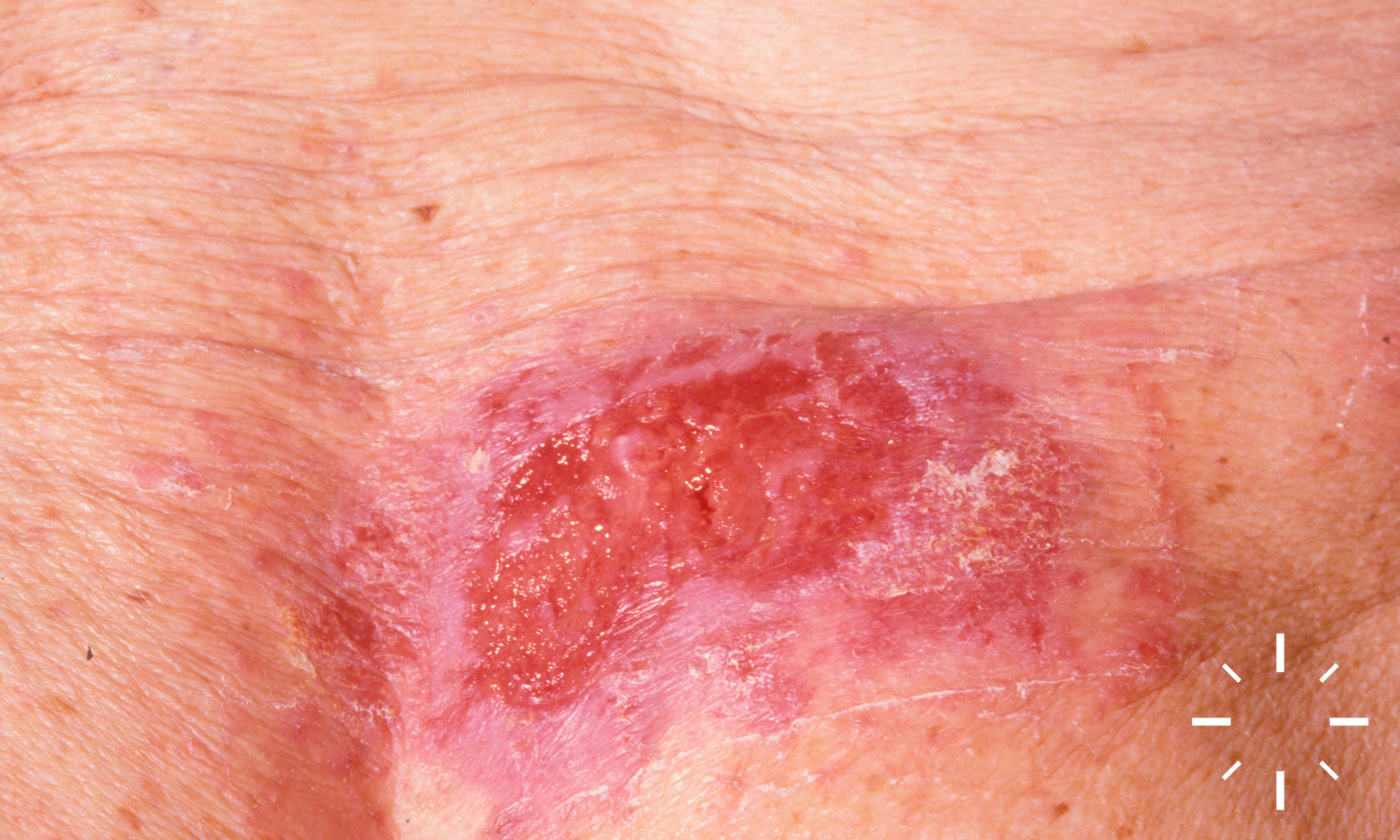
Basalzellkarzinom (incl. Subtypen)
Zuletzt aktualisiert: 2024-10-25
Autor(en): Anzengruber F., Navarini A.
ICD11: 2C32.Z








































































































1/128