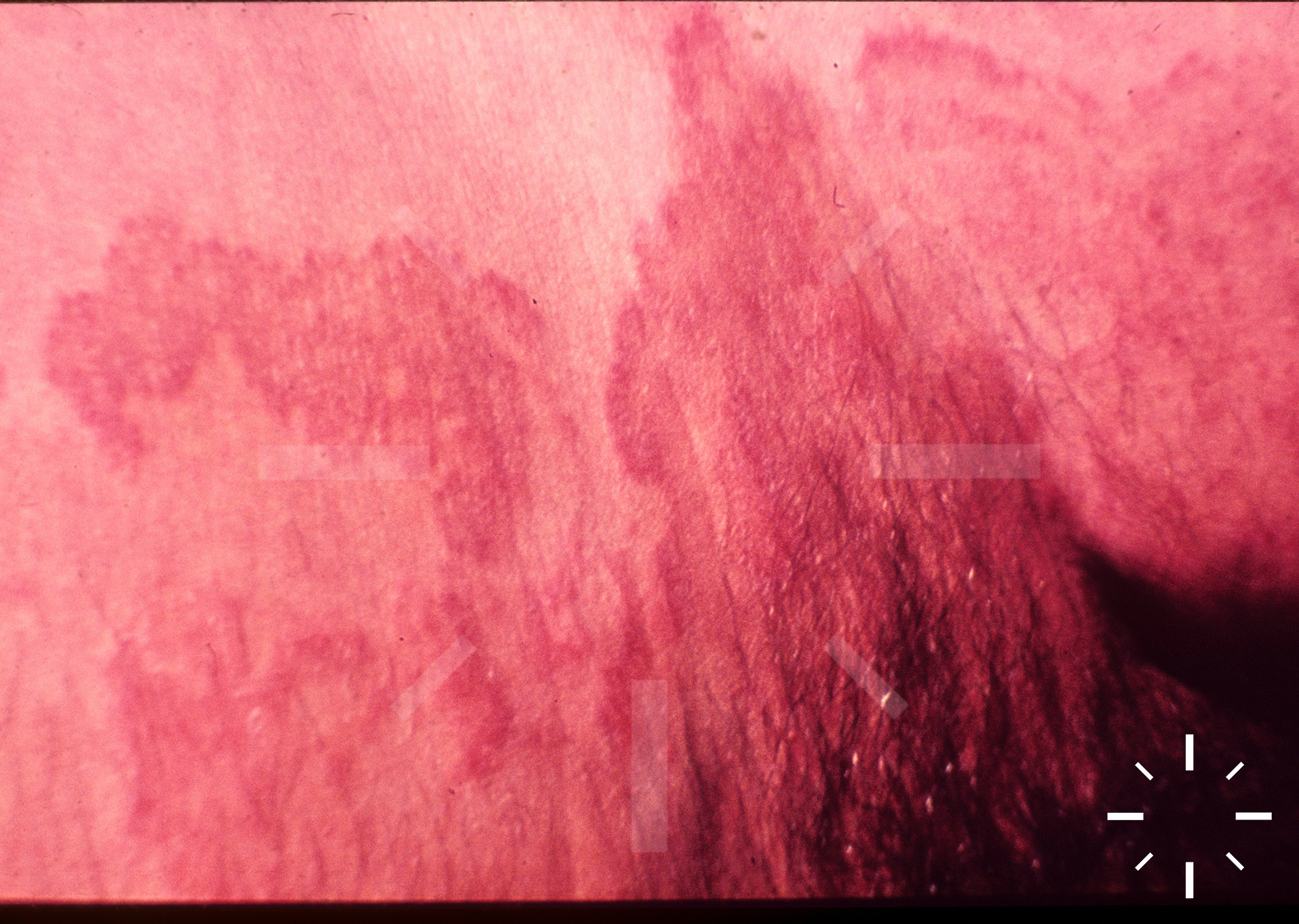
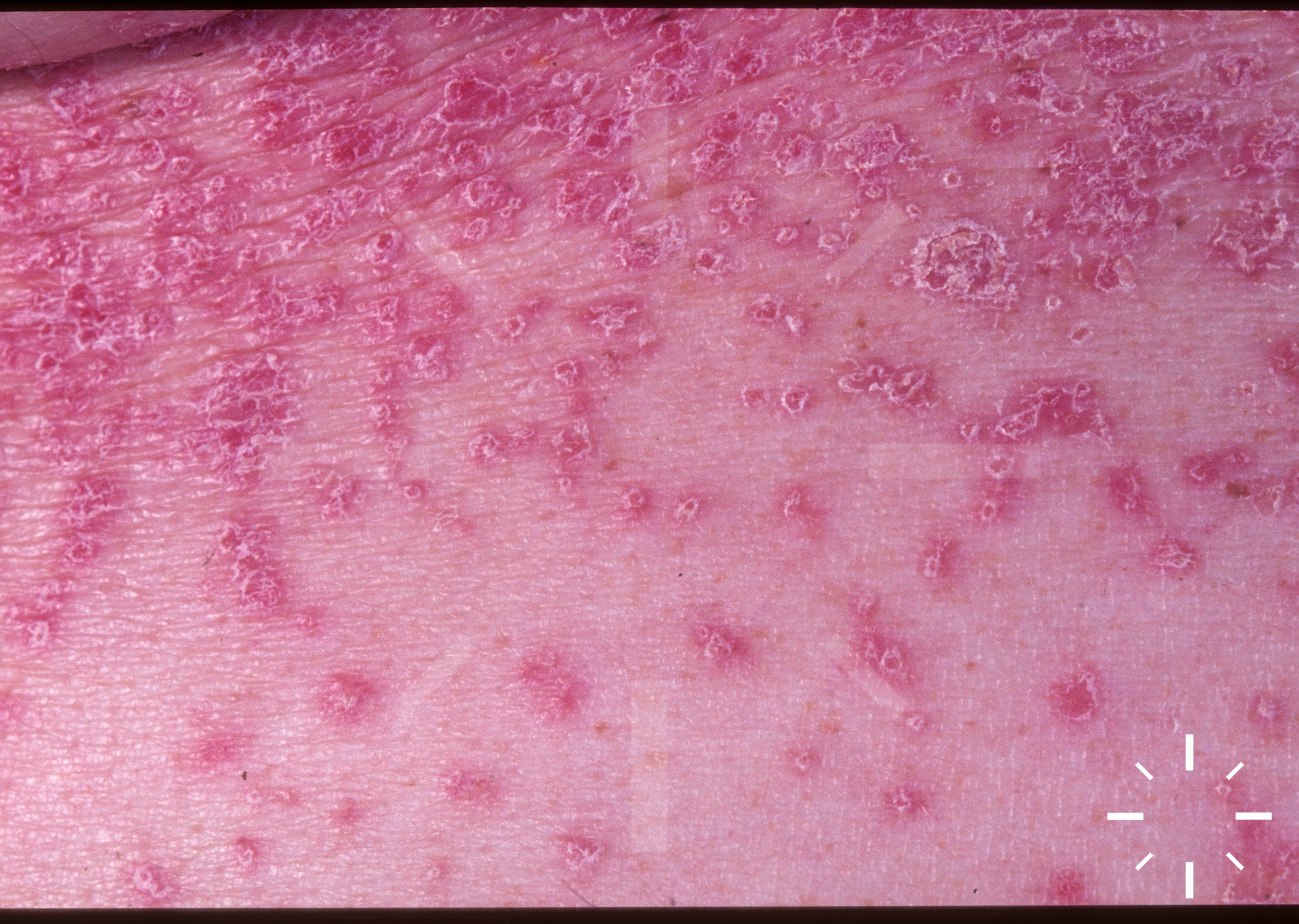
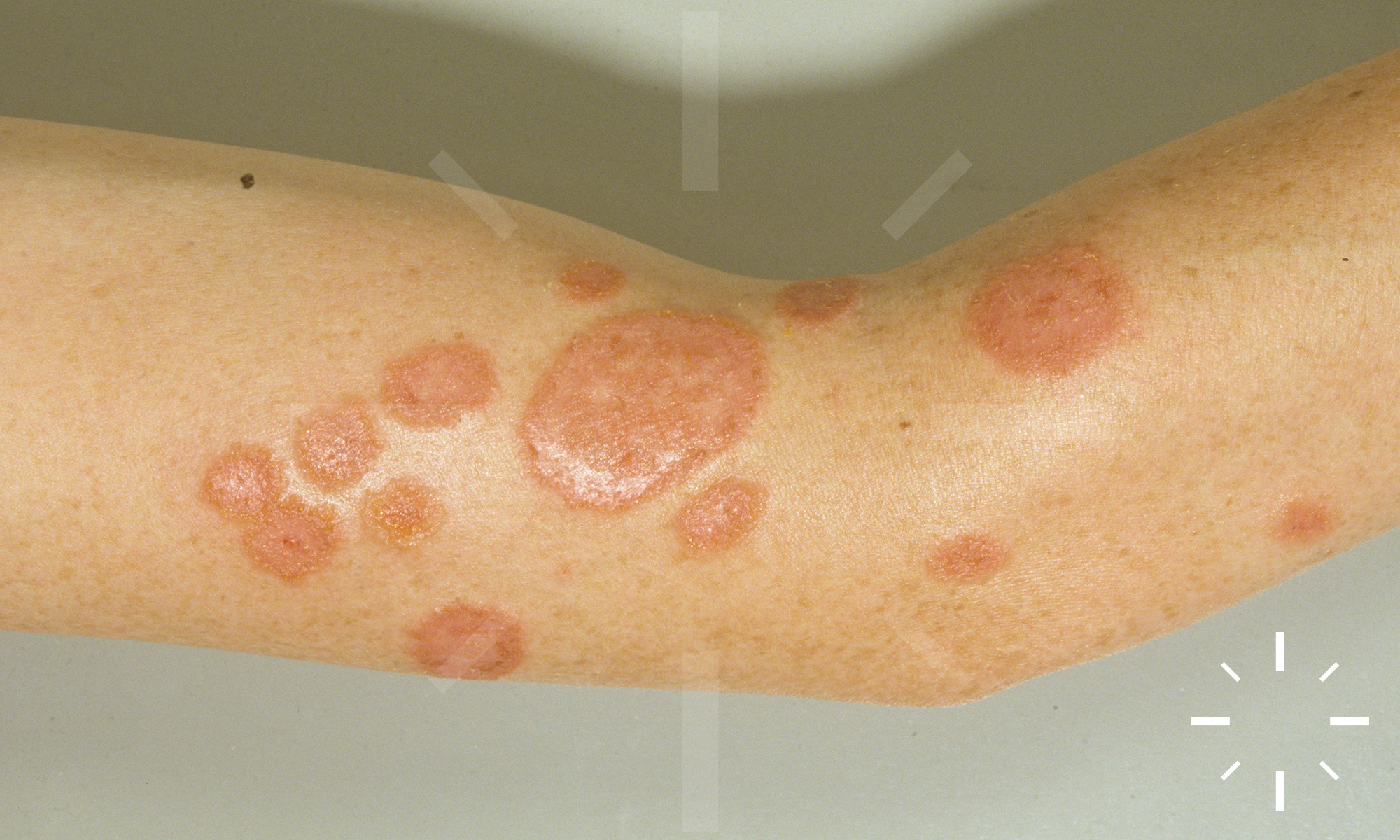
Tinea corporis (mycosis)
Last Updated: 2025-02-11
Author(s): Anzengruber F.
ICD11: 1F28.Y


































1/37